




Jonathan Ryder, MD
@jonathanrydermd.bsky.social
Adult ID and Assistant Prof at UNMC | Former IUSM IM & Truman State | Abx Stewie, Infxn Prevention, Digital MedEd, Podcasts, Medical History, Reading Non-Fiction, Running/Cycling | Posts are mine
Reposted by Jonathan Ryder, MD

🆕 Episode of Breakpoints:
Our host Dr, Ryan Moenster is back and breaking down the recently published ATS pneumonia guidelines — what’s pneu and what it means for your antimicrobial game! Dr Hartlage is back to join the conversation, plus fresh takes from Dr. Weissma and Angelo.
🎧 sidp.pinecast.co
Our host Dr, Ryan Moenster is back and breaking down the recently published ATS pneumonia guidelines — what’s pneu and what it means for your antimicrobial game! Dr Hartlage is back to join the conversation, plus fresh takes from Dr. Weissma and Angelo.
🎧 sidp.pinecast.co

November 28, 2025 at 10:01 AM
🆕 Episode of Breakpoints:
Our host Dr, Ryan Moenster is back and breaking down the recently published ATS pneumonia guidelines — what’s pneu and what it means for your antimicrobial game! Dr Hartlage is back to join the conversation, plus fresh takes from Dr. Weissma and Angelo.
🎧 sidp.pinecast.co
Our host Dr, Ryan Moenster is back and breaking down the recently published ATS pneumonia guidelines — what’s pneu and what it means for your antimicrobial game! Dr Hartlage is back to join the conversation, plus fresh takes from Dr. Weissma and Angelo.
🎧 sidp.pinecast.co
Reposted by Jonathan Ryder, MD

Five subphenotypes of Staphylococcus aureus bacteremia (SAB) were identified in diverse cohorts: 40.2% had MRSA. 90-day mortality was highest in subphenotype A. 🦠💔##idsky
Reproducible identification of Staphylococcus aureus bacteremia clinical subphenotypes
Clinical heterogeneity in Staphylococcus aureus bacteremia (SAB) complicates clinical management and research. We have previously identified five clinically distinct subphenotypes of SAB associated with differences in outcomes and response to adjunctive rifampicin. Here, we aimed to identify these subphenotypes in geographically diverse observational cohorts, including a higher prevalence of methicillin-resistant S. aureus (MRSA) bacteremia and the USA300 clone.MethodsWe studied three cohorts of adults with SAB from observational studies: a UK retrospective study (Edinburgh cohort 2, n=463); a Dutch prospective study (IDISA, n=490); and a USA prospective study (SABG-PCS, n=755). Subphenotypes were identified from routinely available clinical data using latent class analysis.ResultsPatients from the SABG-PCS cohort had greater multimorbidity and more MRSA bacteremia (40.2%, 303/755), including infection with the USA300 clone (14.7%, 111/755). Five distinct subphenotypes were identified in each cohort: (A) older age and cardio-metabolic multimorbidity; (B) nosocomial acquisition and intravenous catheter portal of entry; (C) community acquisition and metastatic infection; (D) chronic kidney disease; and (E) younger age, injection drug use, and metastatic infection. Bacterial genotypes varied substantially between the Edinburgh 2 and SABG-PCS cohorts but did not differ between subphenotypes within each cohort. 90-day mortality was highest in subphenotype A, and persistent bacteremia in subphenotypes C and E.ConclusionsWe have reproducibly identified five clinical subphenotypes of SAB in observational cohorts including diverse bacterial genetic lineages and a cohort with a high prevalence of MRSA and USA300 bacteremia. These robustly reproducible clinical subphenotypes provide a framework to rationalize the heterogeneity intrinsic to SAB.
academic.oup.com
November 27, 2025 at 11:30 PM
Five subphenotypes of Staphylococcus aureus bacteremia (SAB) were identified in diverse cohorts: 40.2% had MRSA. 90-day mortality was highest in subphenotype A. 🦠💔##idsky
Reposted by Jonathan Ryder, MD

📣 New #Communicable drops Mon 1 Dec!
Annie Joseph & Angela Huttner host Dan Morgan (USA) & Valerie Vaughn (USA) to discuss diagnostic stewardship - what it means and why we should do it.
#IDSky #clinmicro #MedSky #meded
Annie Joseph & Angela Huttner host Dan Morgan (USA) & Valerie Vaughn (USA) to discuss diagnostic stewardship - what it means and why we should do it.
#IDSky #clinmicro #MedSky #meded

November 27, 2025 at 10:40 AM
📣 New #Communicable drops Mon 1 Dec!
Annie Joseph & Angela Huttner host Dan Morgan (USA) & Valerie Vaughn (USA) to discuss diagnostic stewardship - what it means and why we should do it.
#IDSky #clinmicro #MedSky #meded
Annie Joseph & Angela Huttner host Dan Morgan (USA) & Valerie Vaughn (USA) to discuss diagnostic stewardship - what it means and why we should do it.
#IDSky #clinmicro #MedSky #meded
Reposted by Jonathan Ryder, MD
The draft for the 2026 IDSA/ESCMID clinical practice guidelines on 𝘚. 𝘢𝘶𝘳𝘦𝘶𝘴 bacteraemia is now available for public consultation. Get your copy of the manuscript and submit your feedback before 15 December 2025.
https://ow.ly/HZao50XwVYg
#IDSky #clinmicro
https://ow.ly/HZao50XwVYg
#IDSky #clinmicro

November 27, 2025 at 6:35 AM
The draft for the 2026 IDSA/ESCMID clinical practice guidelines on 𝘚. 𝘢𝘶𝘳𝘦𝘶𝘴 bacteraemia is now available for public consultation. Get your copy of the manuscript and submit your feedback before 15 December 2025.
https://ow.ly/HZao50XwVYg
#IDSky #clinmicro
https://ow.ly/HZao50XwVYg
#IDSky #clinmicro
Reposted by Jonathan Ryder, MD

So happy to see this paper out after a lot of persistence from Shardul Rathod @hannahnam.bsky.social @ucirvine.bsky.social.
Over a 10 yr period, 6.6% of Flu cases, 12.2% of RSV cases, and 10.9% of PIV cases were Hosp-Acquired. Most in ICH.
onlinelibrary.wiley.com/doi/10.1111/...
Over a 10 yr period, 6.6% of Flu cases, 12.2% of RSV cases, and 10.9% of PIV cases were Hosp-Acquired. Most in ICH.
onlinelibrary.wiley.com/doi/10.1111/...

Hospital‐Acquired Respiratory Viral Infections (HA‐RVIs) over 10 Years Disproportionally Affect the Immunocompromised
The incidence of HA-Flu/RSV/PIV is associated with patients at high risk of developing RVI complications such as oncology and SCT patients and that most HA cases occur during winter respiratory virus...
onlinelibrary.wiley.com
November 25, 2025 at 10:29 PM
So happy to see this paper out after a lot of persistence from Shardul Rathod @hannahnam.bsky.social @ucirvine.bsky.social.
Over a 10 yr period, 6.6% of Flu cases, 12.2% of RSV cases, and 10.9% of PIV cases were Hosp-Acquired. Most in ICH.
onlinelibrary.wiley.com/doi/10.1111/...
Over a 10 yr period, 6.6% of Flu cases, 12.2% of RSV cases, and 10.9% of PIV cases were Hosp-Acquired. Most in ICH.
onlinelibrary.wiley.com/doi/10.1111/...
Reposted by Jonathan Ryder, MD

Can we really be grateful for anything in the ID world in 2025?
Sure -- plenty of great advances!
Here are a half-dozen to celebrate (and be grateful for) in 2025, believe it or not. #idsky
blogs.jwatch.org/hiv-id-obser...
Sure -- plenty of great advances!
Here are a half-dozen to celebrate (and be grateful for) in 2025, believe it or not. #idsky
blogs.jwatch.org/hiv-id-obser...

ID Things to Be Grateful for -- 2025 Edition
Looking back on these annual Thanksgiving posts, I notice an odd pattern: every few years, the intro turns into a kind of apology. As in, Yes, I know the title sounds upbeat, please don’t attack me. T...
blogs.jwatch.org
November 25, 2025 at 2:29 AM
Can we really be grateful for anything in the ID world in 2025?
Sure -- plenty of great advances!
Here are a half-dozen to celebrate (and be grateful for) in 2025, believe it or not. #idsky
blogs.jwatch.org/hiv-id-obser...
Sure -- plenty of great advances!
Here are a half-dozen to celebrate (and be grateful for) in 2025, believe it or not. #idsky
blogs.jwatch.org/hiv-id-obser...
Reposted by Jonathan Ryder, MD

New #LetsTalkID out now!🎙️ @matih-id.bsky.social and @drdemetre.bsky.social explore the current state of public health. They discuss how political pressures and weakened infrastructure have left the system vulnerable, and how this could spark a public health “renaissance."
Transcript: bit.ly/4887CZq
Transcript: bit.ly/4887CZq

From Darkness to Opportunity: Reimagining the Future of Public Health
Mati Hlatshwayo Davis, MD, MPH, FIDSA, and former CDC director Demetre Daskalakis MD, MPH, explore the current state of public health.
bit.ly
November 23, 2025 at 2:11 AM
New #LetsTalkID out now!🎙️ @matih-id.bsky.social and @drdemetre.bsky.social explore the current state of public health. They discuss how political pressures and weakened infrastructure have left the system vulnerable, and how this could spark a public health “renaissance."
Transcript: bit.ly/4887CZq
Transcript: bit.ly/4887CZq
Reposted by Jonathan Ryder, MD
Continuing #WAAW with opportunities in peripartum stewardship, as discussed in our latest podcast: buff.ly/dbhiyQr where @pamipenem.bsky.social and coauthors discuss how QI work builds momentum (and relationships) in this unique population.

Episode 25: Stewardship Opportunities in Peripartum Infections
In this episode of The ASHE Podcast, host Dr. Priya Nori speaks with Dr. Alexia Foy-Crowder, Dr. Pam Bailey, and Dr. Grace Pazienza about their ASHE paper, “Stewardship opportunities in peripartum inf
soundcloud.com
November 23, 2025 at 4:08 PM
Continuing #WAAW with opportunities in peripartum stewardship, as discussed in our latest podcast: buff.ly/dbhiyQr where @pamipenem.bsky.social and coauthors discuss how QI work builds momentum (and relationships) in this unique population.
Reposted by Jonathan Ryder, MD

In the latest episode of The ASHE Podcast, Dr. Priya Nori speaks with the authors of a new paper in ASHE, "Stewardship opportunities in peripartum infections: a review of quality improvement initiatives and future directions".
bit.ly/4rfM8CG
bit.ly/4rfM8CG

November 21, 2025 at 9:55 PM
In the latest episode of The ASHE Podcast, Dr. Priya Nori speaks with the authors of a new paper in ASHE, "Stewardship opportunities in peripartum infections: a review of quality improvement initiatives and future directions".
bit.ly/4rfM8CG
bit.ly/4rfM8CG
Reposted by Jonathan Ryder, MD
Inspired by this rage-inducing ad, I offer 3 big misses on antibiotics that need to die.
paulsaxmd.substack.com/p/three-myth...
paulsaxmd.substack.com/p/three-myth...

Three Myths About Antibiotics We Really Need to Retire
Sneezes, penicillin allergies, and those strangely sacred 5- and 7-day courses.
paulsaxmd.substack.com
November 21, 2025 at 3:53 PM
Inspired by this rage-inducing ad, I offer 3 big misses on antibiotics that need to die.
paulsaxmd.substack.com/p/three-myth...
paulsaxmd.substack.com/p/three-myth...
Reposted by Jonathan Ryder, MD

Is one dose ever enough? The PROSPECTOR 🪓 Trial will answer - A international double blind placebo controlled trial of 1 dose vs 5 day for #penicillinallergy. This week we recruited our 100th patient! 🎉 @thedohertyinst.bsky.social
November 21, 2025 at 11:04 AM
Is one dose ever enough? The PROSPECTOR 🪓 Trial will answer - A international double blind placebo controlled trial of 1 dose vs 5 day for #penicillinallergy. This week we recruited our 100th patient! 🎉 @thedohertyinst.bsky.social
Reposted by Jonathan Ryder, MD
The largest adult #penicillinallergy study ever undertaken - The iNAAN study @thedohertyinst.bsky.social @unimelb.bsky.social - 52 hospitals, 8 countries and over 5000 patients….Real world proof of the safety and effectiveness of inpatient DOC! Stay tuned #AMS folks 👀Results soon!
November 21, 2025 at 11:50 PM
The largest adult #penicillinallergy study ever undertaken - The iNAAN study @thedohertyinst.bsky.social @unimelb.bsky.social - 52 hospitals, 8 countries and over 5000 patients….Real world proof of the safety and effectiveness of inpatient DOC! Stay tuned #AMS folks 👀Results soon!
CDC 1946-2025: R.I.P.
open.substack.com/pub/pauloffi...
open.substack.com/pub/pauloffi...

CDC 1946-2025: R.I.P.
Robert F. Kennedy Jr. has now weaponized the CDC website to promote his anti-vaccine views
open.substack.com
November 21, 2025 at 5:19 AM
CDC 1946-2025: R.I.P.
open.substack.com/pub/pauloffi...
open.substack.com/pub/pauloffi...
Reposted by Jonathan Ryder, MD
Decades of rigorous and scientifically sound research have proven that vaccines do not cause autism. CDC’s decision to change language on its website reversing that finding is reckless & harmful.
Our statement w/ @hivma.bsky.social, APIC, @sheaepi.bsky.social & @sidpharm.bsky.social: bit.ly/3XEc0KH
Our statement w/ @hivma.bsky.social, APIC, @sheaepi.bsky.social & @sidpharm.bsky.social: bit.ly/3XEc0KH

November 21, 2025 at 12:42 AM
Decades of rigorous and scientifically sound research have proven that vaccines do not cause autism. CDC’s decision to change language on its website reversing that finding is reckless & harmful.
Our statement w/ @hivma.bsky.social, APIC, @sheaepi.bsky.social & @sidpharm.bsky.social: bit.ly/3XEc0KH
Our statement w/ @hivma.bsky.social, APIC, @sheaepi.bsky.social & @sidpharm.bsky.social: bit.ly/3XEc0KH
Reposted by Jonathan Ryder, MD

A new NEJM paper just dropped evaluating a quadrivalent modified mRNA (modRNA) influenza vaccine in a phase 3 trial. This is the largest test yet of whether the mRNA platform that transformed COVID-19 vaccination can improve our fight against flu.
www.nejm.org/doi/full/10....
www.nejm.org/doi/full/10....

Efficacy, Immunogenicity, and Safety of Modified mRNA Influenza Vaccine | NEJM
Influenza remains a major health burden despite the use of licensed vaccines. Nucleoside-modified
messenger RNA (modRNA) influenza vaccines have shown promising immunogenicity against
influenza and...
www.nejm.org
November 20, 2025 at 12:26 PM
A new NEJM paper just dropped evaluating a quadrivalent modified mRNA (modRNA) influenza vaccine in a phase 3 trial. This is the largest test yet of whether the mRNA platform that transformed COVID-19 vaccination can improve our fight against flu.
www.nejm.org/doi/full/10....
www.nejm.org/doi/full/10....
Reposted by Jonathan Ryder, MD

Modified mRNA vaccine non-inferior *and* superior to usual quadravalent influenza vaccine in this RCT of 18.5K people during 2022/2023 flu season, relative efficacy 34.5%.
mRNA vaccine with increased local and systemic reactions, AEs similar… #IDSky #vaccines
www.nejm.org/doi/full/10....
mRNA vaccine with increased local and systemic reactions, AEs similar… #IDSky #vaccines
www.nejm.org/doi/full/10....

Efficacy, Immunogenicity, and Safety of Modified mRNA Influenza Vaccine | NEJM
Influenza remains a major health burden despite the use of licensed vaccines. Nucleoside-modified messenger RNA (modRNA) influenza vaccines have shown promising immunogenicity against influenza and...
www.nejm.org
November 19, 2025 at 11:21 PM
Modified mRNA vaccine non-inferior *and* superior to usual quadravalent influenza vaccine in this RCT of 18.5K people during 2022/2023 flu season, relative efficacy 34.5%.
mRNA vaccine with increased local and systemic reactions, AEs similar… #IDSky #vaccines
www.nejm.org/doi/full/10....
mRNA vaccine with increased local and systemic reactions, AEs similar… #IDSky #vaccines
www.nejm.org/doi/full/10....
Reposted by Jonathan Ryder, MD


Reposted by Jonathan Ryder, MD

🆕🔥🦴 Our 2025 Update to @wiki-guidelines.bsky.social for the Management of Pyogenic Osteomyelitis in Adults 🌟 @bradspellberg.bsky.social
🔗 [link] #idsky
www.amjmed.com/article/S000...
🔗 [link] #idsky
www.amjmed.com/article/S000...

November 19, 2025 at 4:25 PM
🆕🔥🦴 Our 2025 Update to @wiki-guidelines.bsky.social for the Management of Pyogenic Osteomyelitis in Adults 🌟 @bradspellberg.bsky.social
🔗 [link] #idsky
www.amjmed.com/article/S000...
🔗 [link] #idsky
www.amjmed.com/article/S000...
Reposted by Jonathan Ryder, MD

The next #MedEd game for #WAAW2025 is here! Can you find the four groups of four items that belong together? 🧩🤔
Play Infectious Connections today: connections.firstline.org
Discover the engaging educational content crafted by Shaqil Peermohamed, MD! #IDSky #PharmSky #AMSSKy
Play Infectious Connections today: connections.firstline.org
Discover the engaging educational content crafted by Shaqil Peermohamed, MD! #IDSky #PharmSky #AMSSKy

November 17, 2025 at 2:26 PM
Reposted by Jonathan Ryder, MD
USAAW urges proper antibiotic & antifungal use to protect people, animals, plants & our environment. This year’s theme, Fighting Antimicrobial Resistance Takes All of Us, reminds us our health is connected. Together we can improve prescribing and fight antimicrobial resistance.
November 18, 2025 at 3:26 PM
USAAW urges proper antibiotic & antifungal use to protect people, animals, plants & our environment. This year’s theme, Fighting Antimicrobial Resistance Takes All of Us, reminds us our health is connected. Together we can improve prescribing and fight antimicrobial resistance.
Reposted by Jonathan Ryder, MD
Trying to remember which bacteria have bipolar staining? Love this slide from @iuidfellowship.bsky.social
- Yersinia pestis
- Vibrio parahemolyticus
- Burkholderia mallei and pseudomallei
- Haemophilus ducreyi
- Klebsiella granulomatis
#IDSky
- Yersinia pestis
- Vibrio parahemolyticus
- Burkholderia mallei and pseudomallei
- Haemophilus ducreyi
- Klebsiella granulomatis
#IDSky

November 18, 2025 at 12:55 AM
Trying to remember which bacteria have bipolar staining? Love this slide from @iuidfellowship.bsky.social
- Yersinia pestis
- Vibrio parahemolyticus
- Burkholderia mallei and pseudomallei
- Haemophilus ducreyi
- Klebsiella granulomatis
#IDSky
- Yersinia pestis
- Vibrio parahemolyticus
- Burkholderia mallei and pseudomallei
- Haemophilus ducreyi
- Klebsiella granulomatis
#IDSky
Reposted by Jonathan Ryder, MD

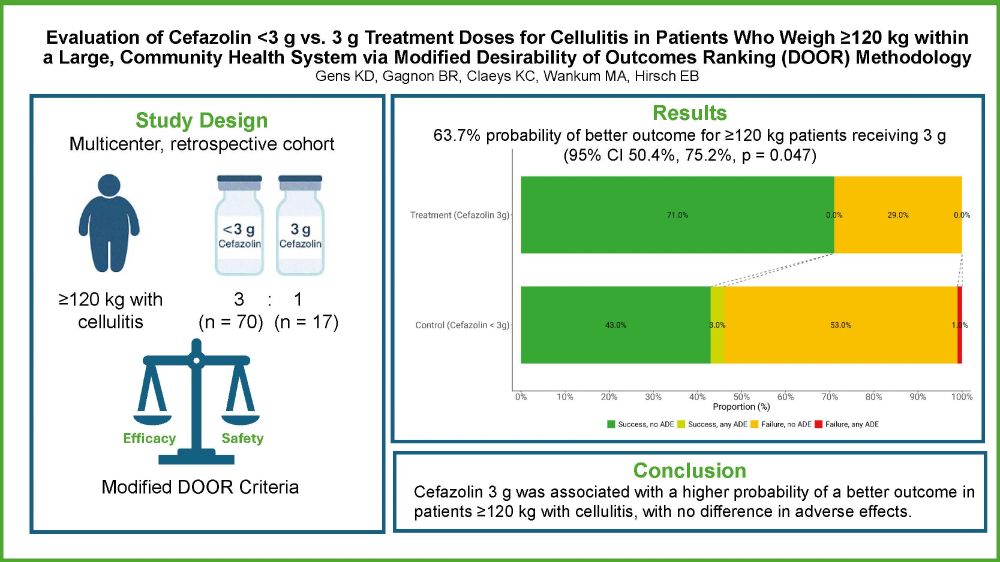
📢 Excited to announce our new research is now published in the JIC! 🎉
🔍 What were we seeing? 3 g of cefazolin for cellulitis in obese patients.
🚪 Why DOOR? It combines efficacy and safety outcomes.
💡 What did we find? 3 g might be a good idea.
lnkd.in/gbP4sx_7
@ebhirsch.bsky.social
🔍 What were we seeing? 3 g of cefazolin for cellulitis in obese patients.
🚪 Why DOOR? It combines efficacy and safety outcomes.
💡 What did we find? 3 g might be a good idea.
lnkd.in/gbP4sx_7
@ebhirsch.bsky.social
November 17, 2025 at 5:11 PM
📢 Excited to announce our new research is now published in the JIC! 🎉
🔍 What were we seeing? 3 g of cefazolin for cellulitis in obese patients.
🚪 Why DOOR? It combines efficacy and safety outcomes.
💡 What did we find? 3 g might be a good idea.
lnkd.in/gbP4sx_7
@ebhirsch.bsky.social
🔍 What were we seeing? 3 g of cefazolin for cellulitis in obese patients.
🚪 Why DOOR? It combines efficacy and safety outcomes.
💡 What did we find? 3 g might be a good idea.
lnkd.in/gbP4sx_7
@ebhirsch.bsky.social
Reposted by Jonathan Ryder, MD

Fascinating article on the history of syphilis:
“English people called it the
“Spanish disease”… the Spanish called it mal inglés.
The Dutch called it “Spanish smallpox”
The Russians blamed the Poles, and the Turks referred to it as the “Christian disease””
#IDSky
academic.oup.com/jid/advance-...
“English people called it the
“Spanish disease”… the Spanish called it mal inglés.
The Dutch called it “Spanish smallpox”
The Russians blamed the Poles, and the Turks referred to it as the “Christian disease””
#IDSky
academic.oup.com/jid/advance-...

Syphilis Transmission: Contagion of Bodies and Words
Syphilis, infection caused by Treponema pallidum, occurred in Naples and in Europe in the late 15th century impacting on people’s lives. Here, we explored
academic.oup.com
November 16, 2025 at 3:56 AM
Fascinating article on the history of syphilis:
“English people called it the
“Spanish disease”… the Spanish called it mal inglés.
The Dutch called it “Spanish smallpox”
The Russians blamed the Poles, and the Turks referred to it as the “Christian disease””
#IDSky
academic.oup.com/jid/advance-...
“English people called it the
“Spanish disease”… the Spanish called it mal inglés.
The Dutch called it “Spanish smallpox”
The Russians blamed the Poles, and the Turks referred to it as the “Christian disease””
#IDSky
academic.oup.com/jid/advance-...
Reposted by Jonathan Ryder, MD

Congratulations to Hemant Roy, MD, on his appointment as the new chair of the UNMC Department of Internal Medicine!
More:
www.unmc.edu/newsroom/202...
More:
www.unmc.edu/newsroom/202...

Hemant Roy, MD, announced as internal medicine chair
Dr. Roy, currently at Ben Taub Hospital and Baylor College of Medicine, is a former UNMC faculty member with demonstrated expertise.
www.unmc.edu
November 14, 2025 at 6:08 PM
Congratulations to Hemant Roy, MD, on his appointment as the new chair of the UNMC Department of Internal Medicine!
More:
www.unmc.edu/newsroom/202...
More:
www.unmc.edu/newsroom/202...
Reposted by Jonathan Ryder, MD

Our new paper out: AI boosted our genomic surveillance investigations by finding 37 missed transmission routes and reaching >90% sensitivity in key scenarios.
AI + WGS can speed outbreak reviews and help IP teams act faster #IDSky
Genomic surveillance is a key must!
📃: doi.org/10.1017/ice....
AI + WGS can speed outbreak reviews and help IP teams act faster #IDSky
Genomic surveillance is a key must!
📃: doi.org/10.1017/ice....




November 14, 2025 at 3:09 PM
Our new paper out: AI boosted our genomic surveillance investigations by finding 37 missed transmission routes and reaching >90% sensitivity in key scenarios.
AI + WGS can speed outbreak reviews and help IP teams act faster #IDSky
Genomic surveillance is a key must!
📃: doi.org/10.1017/ice....
AI + WGS can speed outbreak reviews and help IP teams act faster #IDSky
Genomic surveillance is a key must!
📃: doi.org/10.1017/ice....