



Lea Alhilali, MD
@teachplaygrub.bsky.social
Senior editor American Journal of Neuroradiology; Associate Editor, Radiographics; Associate Editor, Radiology; Deputy Editor, Clinical Neuroimaging.
I try to make learning neuroimaging and neuroanatomy fun. If I can make you laugh, I can help you learn.
I try to make learning neuroimaging and neuroanatomy fun. If I can make you laugh, I can help you learn.
Are you right when it’s bright?
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD
January 23, 2025 at 5:00 PM
Are you right when it’s bright?
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD
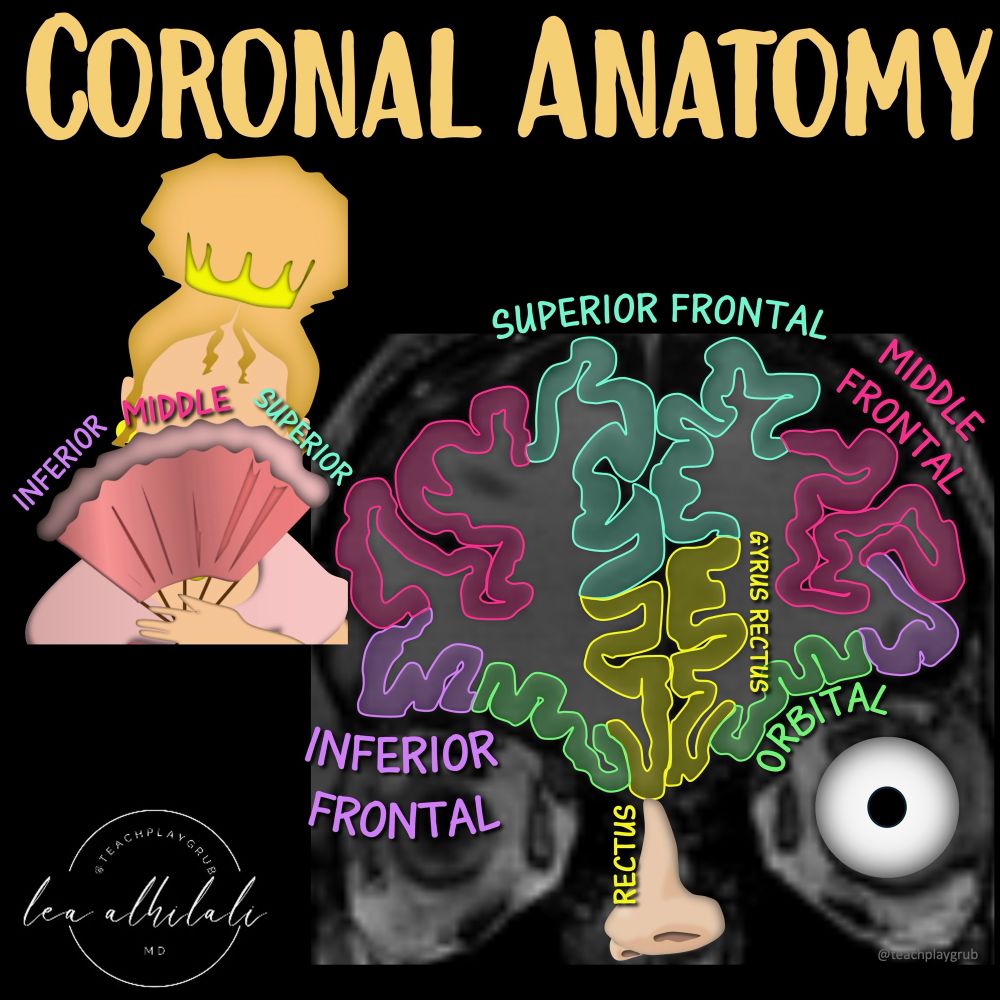
1/Have you been cutting corners when it comes to coronal anatomy?
Do you just say a lesion is in the inferior frontal region & hope no one asks for details?
It’s time to turn the corner on coronal anatomy
Open this thread for an easy way to remember this frontal anatomy you need to know!
Do you just say a lesion is in the inferior frontal region & hope no one asks for details?
It’s time to turn the corner on coronal anatomy
Open this thread for an easy way to remember this frontal anatomy you need to know!
January 21, 2025 at 4:38 PM
1/Have you been cutting corners when it comes to coronal anatomy?
Do you just say a lesion is in the inferior frontal region & hope no one asks for details?
It’s time to turn the corner on coronal anatomy
Open this thread for an easy way to remember this frontal anatomy you need to know!
Do you just say a lesion is in the inferior frontal region & hope no one asks for details?
It’s time to turn the corner on coronal anatomy
Open this thread for an easy way to remember this frontal anatomy you need to know!
1/
“Tell me where it hurts”
How back pain radiates can tell you where a lesion is—if you know where to look!
Do YOU know where to look?
Open this thread to see how to remember lumbar radicular pain distributions!
And keep this cheat sheet as a BACKUP for when you are dealing w/back pain!
“Tell me where it hurts”
How back pain radiates can tell you where a lesion is—if you know where to look!
Do YOU know where to look?
Open this thread to see how to remember lumbar radicular pain distributions!
And keep this cheat sheet as a BACKUP for when you are dealing w/back pain!

January 16, 2025 at 3:55 PM
1/
“Tell me where it hurts”
How back pain radiates can tell you where a lesion is—if you know where to look!
Do YOU know where to look?
Open this thread to see how to remember lumbar radicular pain distributions!
And keep this cheat sheet as a BACKUP for when you are dealing w/back pain!
“Tell me where it hurts”
How back pain radiates can tell you where a lesion is—if you know where to look!
Do YOU know where to look?
Open this thread to see how to remember lumbar radicular pain distributions!
And keep this cheat sheet as a BACKUP for when you are dealing w/back pain!
1/Sink or swim!
Brain is swimming in CSF!
CSF is key for protection, buoyancy, & hormone/waste transport
Most know basic ventricular anatomy, but not subarachnoid anatomy
How many cisterns do YOU know?
Open this thread for a quick guide to the key midline cisterns & what to know for each!
Brain is swimming in CSF!
CSF is key for protection, buoyancy, & hormone/waste transport
Most know basic ventricular anatomy, but not subarachnoid anatomy
How many cisterns do YOU know?
Open this thread for a quick guide to the key midline cisterns & what to know for each!

January 13, 2025 at 3:43 PM
1/Sink or swim!
Brain is swimming in CSF!
CSF is key for protection, buoyancy, & hormone/waste transport
Most know basic ventricular anatomy, but not subarachnoid anatomy
How many cisterns do YOU know?
Open this thread for a quick guide to the key midline cisterns & what to know for each!
Brain is swimming in CSF!
CSF is key for protection, buoyancy, & hormone/waste transport
Most know basic ventricular anatomy, but not subarachnoid anatomy
How many cisterns do YOU know?
Open this thread for a quick guide to the key midline cisterns & what to know for each!
1/Just because it’s called SMALL vessel disease doesn’t mean it doesn’t have a BIG impact!
Small vessel disease (SVD) is a BIG contributor to vascular dementia, along w/large vessel cortical infarcts
Do YOU know all the faces of small vessel disease?
Open the thread for what you need to know!
Small vessel disease (SVD) is a BIG contributor to vascular dementia, along w/large vessel cortical infarcts
Do YOU know all the faces of small vessel disease?
Open the thread for what you need to know!

January 10, 2025 at 3:57 PM
1/Just because it’s called SMALL vessel disease doesn’t mean it doesn’t have a BIG impact!
Small vessel disease (SVD) is a BIG contributor to vascular dementia, along w/large vessel cortical infarcts
Do YOU know all the faces of small vessel disease?
Open the thread for what you need to know!
Small vessel disease (SVD) is a BIG contributor to vascular dementia, along w/large vessel cortical infarcts
Do YOU know all the faces of small vessel disease?
Open the thread for what you need to know!
Is looking at dementia PETs one of your PET peeves?
Main patterns
🔹AD
Nike swoosh—if you see it, just call it!
🔹DLB
Hypometabolism looks like an L. L=Lewy
🔹FTD
Ant cingulate role makes an f. f=ftd
🔹Posterior cortical atrophy
Anterior temporal sparing makes a C=pCa
🔹Vascular dementia
Wedge shaped Vs
Main patterns
🔹AD
Nike swoosh—if you see it, just call it!
🔹DLB
Hypometabolism looks like an L. L=Lewy
🔹FTD
Ant cingulate role makes an f. f=ftd
🔹Posterior cortical atrophy
Anterior temporal sparing makes a C=pCa
🔹Vascular dementia
Wedge shaped Vs
January 9, 2025 at 6:14 PM
Is looking at dementia PETs one of your PET peeves?
Main patterns
🔹AD
Nike swoosh—if you see it, just call it!
🔹DLB
Hypometabolism looks like an L. L=Lewy
🔹FTD
Ant cingulate role makes an f. f=ftd
🔹Posterior cortical atrophy
Anterior temporal sparing makes a C=pCa
🔹Vascular dementia
Wedge shaped Vs
Main patterns
🔹AD
Nike swoosh—if you see it, just call it!
🔹DLB
Hypometabolism looks like an L. L=Lewy
🔹FTD
Ant cingulate role makes an f. f=ftd
🔹Posterior cortical atrophy
Anterior temporal sparing makes a C=pCa
🔹Vascular dementia
Wedge shaped Vs
Can you only remember temporal anatomy temporarily?
It looks like a parfait!
Heschl’s is strawberry on top
🔸Heschl sounds like bushel—& bushels=fruit
Parfait layers=sup, mid, & inf gyri
Glass stem is fusiform gyrus
🔸Stem has fusiform shape!
Now your understanding will be, well, parfait!!
It looks like a parfait!
Heschl’s is strawberry on top
🔸Heschl sounds like bushel—& bushels=fruit
Parfait layers=sup, mid, & inf gyri
Glass stem is fusiform gyrus
🔸Stem has fusiform shape!
Now your understanding will be, well, parfait!!

January 8, 2025 at 3:14 PM
Can you only remember temporal anatomy temporarily?
It looks like a parfait!
Heschl’s is strawberry on top
🔸Heschl sounds like bushel—& bushels=fruit
Parfait layers=sup, mid, & inf gyri
Glass stem is fusiform gyrus
🔸Stem has fusiform shape!
Now your understanding will be, well, parfait!!
It looks like a parfait!
Heschl’s is strawberry on top
🔸Heschl sounds like bushel—& bushels=fruit
Parfait layers=sup, mid, & inf gyri
Glass stem is fusiform gyrus
🔸Stem has fusiform shape!
Now your understanding will be, well, parfait!!
Does trying to figure out aphasia leave you speechless?
At a loss for words for aphasia types?
Remember 3 ?'s:
1. Fluency? Nonfluency=FRONTAL, ant. to fissure of Rolando
2. Comprehension? Impaired=TEMPOROPARIETAL
3. Repetition? Impaired=core PERISYLVIAN
Answers give aphasia type & location!
At a loss for words for aphasia types?
Remember 3 ?'s:
1. Fluency? Nonfluency=FRONTAL, ant. to fissure of Rolando
2. Comprehension? Impaired=TEMPOROPARIETAL
3. Repetition? Impaired=core PERISYLVIAN
Answers give aphasia type & location!

January 6, 2025 at 4:42 PM
Does trying to figure out aphasia leave you speechless?
At a loss for words for aphasia types?
Remember 3 ?'s:
1. Fluency? Nonfluency=FRONTAL, ant. to fissure of Rolando
2. Comprehension? Impaired=TEMPOROPARIETAL
3. Repetition? Impaired=core PERISYLVIAN
Answers give aphasia type & location!
At a loss for words for aphasia types?
Remember 3 ?'s:
1. Fluency? Nonfluency=FRONTAL, ant. to fissure of Rolando
2. Comprehension? Impaired=TEMPOROPARIETAL
3. Repetition? Impaired=core PERISYLVIAN
Answers give aphasia type & location!
Are you right when it’s bright?
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD

January 3, 2025 at 4:56 PM
Are you right when it’s bright?
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD
Bright cortex on DWI is classically anoxic injury
But mimics exist!
6 patterns
-Cortex+deep gray
-Diffuse Cortex
-Focal Cortex
-Limbic
-Deep gray
-WM
Ask 3 ?’s:
-Acute or chronic?
-Acute=metabolic & anoxic. Sz & encephalitis rarer & focal
-Chronic, think CJD
It literally took my radiologist husband a full minute to figure out what was wrong about this picture!
How long will it take YOU??
And can you spot the abnormality?
Here’s to a year of high resolutions—both in imaging and for New Year’s!
Wishing you all the best in 2025!
How long will it take YOU??
And can you spot the abnormality?
Here’s to a year of high resolutions—both in imaging and for New Year’s!
Wishing you all the best in 2025!

January 1, 2025 at 7:38 PM
It literally took my radiologist husband a full minute to figure out what was wrong about this picture!
How long will it take YOU??
And can you spot the abnormality?
Here’s to a year of high resolutions—both in imaging and for New Year’s!
Wishing you all the best in 2025!
How long will it take YOU??
And can you spot the abnormality?
Here’s to a year of high resolutions—both in imaging and for New Year’s!
Wishing you all the best in 2025!
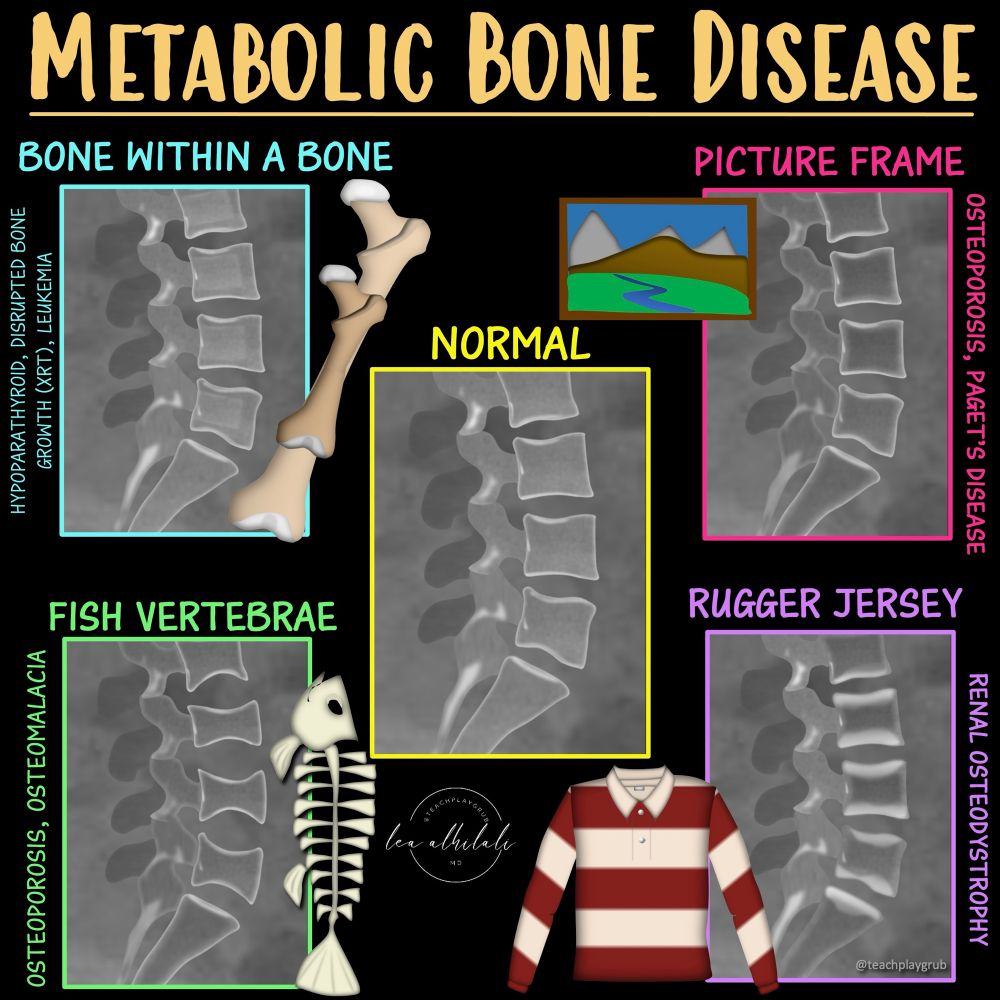
Can’t metabolize all the metabolic bone diseases?
When you see weird bones, do you just say, “suggestive of metabolic bone disease” & hope no one ask questions?
Metabolic disease are complex but a few are a slam dunk
Bookmark this figure for the 4 classic xray patterns you NEED to know!
When you see weird bones, do you just say, “suggestive of metabolic bone disease” & hope no one ask questions?
Metabolic disease are complex but a few are a slam dunk
Bookmark this figure for the 4 classic xray patterns you NEED to know!
December 31, 2024 at 12:20 PM
Can’t metabolize all the metabolic bone diseases?
When you see weird bones, do you just say, “suggestive of metabolic bone disease” & hope no one ask questions?
Metabolic disease are complex but a few are a slam dunk
Bookmark this figure for the 4 classic xray patterns you NEED to know!
When you see weird bones, do you just say, “suggestive of metabolic bone disease” & hope no one ask questions?
Metabolic disease are complex but a few are a slam dunk
Bookmark this figure for the 4 classic xray patterns you NEED to know!
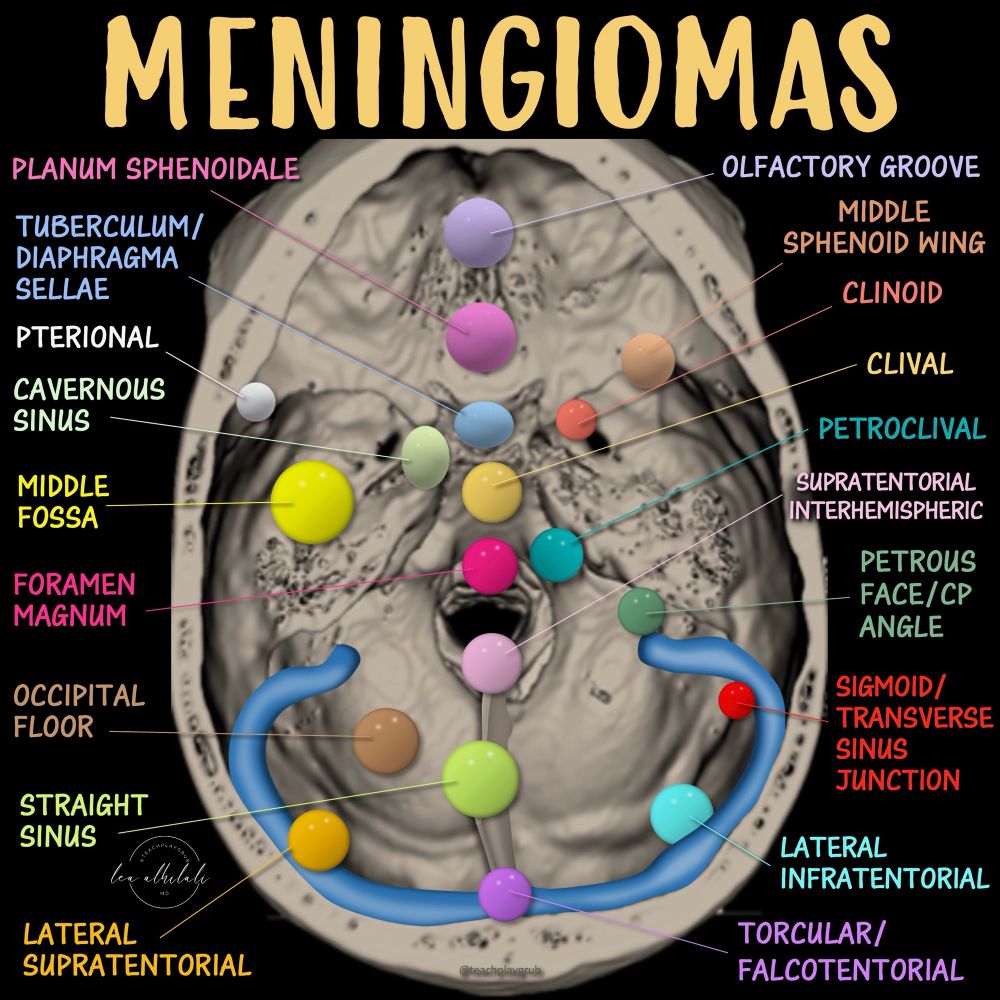
1/ How durable is your knowledge of dural lesions?
How’s your knowledge base of the skull base?
Know the difference between petroclival & petrous face? Middle fossa & middle sphenoid wing? Clinoid & clivus?
Here is a map of the names of skull base meningiomas. How many do you know?
How’s your knowledge base of the skull base?
Know the difference between petroclival & petrous face? Middle fossa & middle sphenoid wing? Clinoid & clivus?
Here is a map of the names of skull base meningiomas. How many do you know?
December 30, 2024 at 12:19 PM
1/ How durable is your knowledge of dural lesions?
How’s your knowledge base of the skull base?
Know the difference between petroclival & petrous face? Middle fossa & middle sphenoid wing? Clinoid & clivus?
Here is a map of the names of skull base meningiomas. How many do you know?
How’s your knowledge base of the skull base?
Know the difference between petroclival & petrous face? Middle fossa & middle sphenoid wing? Clinoid & clivus?
Here is a map of the names of skull base meningiomas. How many do you know?
1/Knowing spinal arterial anatomy is a given.
Knowing spinal venous anatomy is next level
Vertebral venous plexus can be both good & evil--good for collaterals, bad for tumor spread, infxn, & emboli...and spinal CSF fistulas!
Here’s the anatomy you MUST know if you are doing spine
Knowing spinal venous anatomy is next level
Vertebral venous plexus can be both good & evil--good for collaterals, bad for tumor spread, infxn, & emboli...and spinal CSF fistulas!
Here’s the anatomy you MUST know if you are doing spine

December 27, 2024 at 6:48 PM
1/Knowing spinal arterial anatomy is a given.
Knowing spinal venous anatomy is next level
Vertebral venous plexus can be both good & evil--good for collaterals, bad for tumor spread, infxn, & emboli...and spinal CSF fistulas!
Here’s the anatomy you MUST know if you are doing spine
Knowing spinal venous anatomy is next level
Vertebral venous plexus can be both good & evil--good for collaterals, bad for tumor spread, infxn, & emboli...and spinal CSF fistulas!
Here’s the anatomy you MUST know if you are doing spine
Wish that your knowledge of autoimmune encephalitis was automatic?
Do you feel in limbo when it comes to the causes of limbic encephalitis?
Do you know the causes? Or the other patterns of autoimmune encephalitis?
Here’s a short video and some hints to help you figure it all out!
Do you feel in limbo when it comes to the causes of limbic encephalitis?
Do you know the causes? Or the other patterns of autoimmune encephalitis?
Here’s a short video and some hints to help you figure it all out!
December 26, 2024 at 6:55 PM
Wish that your knowledge of autoimmune encephalitis was automatic?
Do you feel in limbo when it comes to the causes of limbic encephalitis?
Do you know the causes? Or the other patterns of autoimmune encephalitis?
Here’s a short video and some hints to help you figure it all out!
Do you feel in limbo when it comes to the causes of limbic encephalitis?
Do you know the causes? Or the other patterns of autoimmune encephalitis?
Here’s a short video and some hints to help you figure it all out!
1/Season’s Greetings & Happy Arteries!
Have you ever noticed how the cerebral arteries branch just like the antlers of a deer?
Coincidence? Or is there a reason?
Have you ever wondered why?
What could drive 2 things so different to look so alike?
Answer may surprise you!!
Have you ever noticed how the cerebral arteries branch just like the antlers of a deer?
Coincidence? Or is there a reason?
Have you ever wondered why?
What could drive 2 things so different to look so alike?
Answer may surprise you!!

December 25, 2024 at 9:17 PM
1/Season’s Greetings & Happy Arteries!
Have you ever noticed how the cerebral arteries branch just like the antlers of a deer?
Coincidence? Or is there a reason?
Have you ever wondered why?
What could drive 2 things so different to look so alike?
Answer may surprise you!!
Have you ever noticed how the cerebral arteries branch just like the antlers of a deer?
Coincidence? Or is there a reason?
Have you ever wondered why?
What could drive 2 things so different to look so alike?
Answer may surprise you!!
1/Time to go with the flow!
If you see abnormal vessels, do you say “vascular malformation” & hope the endovascular guy figures it out?
This months AJNR SCANtastic has the latest on cerebrovascular lesions:
www.ajnr.org/content/45/1...
Here’s the cheat sheet of imaging vascular malformations!
If you see abnormal vessels, do you say “vascular malformation” & hope the endovascular guy figures it out?
This months AJNR SCANtastic has the latest on cerebrovascular lesions:
www.ajnr.org/content/45/1...
Here’s the cheat sheet of imaging vascular malformations!

December 20, 2024 at 2:20 PM
1/Time to go with the flow!
If you see abnormal vessels, do you say “vascular malformation” & hope the endovascular guy figures it out?
This months AJNR SCANtastic has the latest on cerebrovascular lesions:
www.ajnr.org/content/45/1...
Here’s the cheat sheet of imaging vascular malformations!
If you see abnormal vessels, do you say “vascular malformation” & hope the endovascular guy figures it out?
This months AJNR SCANtastic has the latest on cerebrovascular lesions:
www.ajnr.org/content/45/1...
Here’s the cheat sheet of imaging vascular malformations!
18/Now you know the pathology of dural AVFs! Hopefully it stays w/you for the duration!
But this only scratches the surface. Follow @theAJNR & check out the article for yourself:
www.ajnr.org/content/45/1...
But this only scratches the surface. Follow @theAJNR & check out the article for yourself:
www.ajnr.org/content/45/1...

December 19, 2024 at 2:25 PM
18/Now you know the pathology of dural AVFs! Hopefully it stays w/you for the duration!
But this only scratches the surface. Follow @theAJNR & check out the article for yourself:
www.ajnr.org/content/45/1...
But this only scratches the surface. Follow @theAJNR & check out the article for yourself:
www.ajnr.org/content/45/1...
17/This begs the question if there is any truly “benign” dAVF
Even w/o high risk of bleeding, this indicates dAVFs cause more damage than we know & cognitive impairment
Should we be treating these more aggressively?

December 19, 2024 at 2:25 PM
17/This begs the question if there is any truly “benign” dAVF
Even w/o high risk of bleeding, this indicates dAVFs cause more damage than we know & cognitive impairment
Should we be treating these more aggressively?
16/But this classification just addresses the risk of bleeding.
Itskeson et al. found 1/2 of dAVF pts had cognitive impairment. While more common w/cortical reflux, even pts w/o reflux had cognitive impairment that improved w/treatment
Itskeson et al. found 1/2 of dAVF pts had cognitive impairment. While more common w/cortical reflux, even pts w/o reflux had cognitive impairment that improved w/treatment

December 19, 2024 at 2:25 PM
16/But this classification just addresses the risk of bleeding.
Itskeson et al. found 1/2 of dAVF pts had cognitive impairment. While more common w/cortical reflux, even pts w/o reflux had cognitive impairment that improved w/treatment
Itskeson et al. found 1/2 of dAVF pts had cognitive impairment. While more common w/cortical reflux, even pts w/o reflux had cognitive impairment that improved w/treatment
15/But instead of memorizing the classification, ask yourself—can the venous outflow handle the flow (dural sinus vs cortical vein) & does it look like it is overwhelmed (venous ectasia)?
This will intuitively lead you to the classification system w/o having to memorize a thing!
This will intuitively lead you to the classification system w/o having to memorize a thing!

December 19, 2024 at 2:25 PM
15/But instead of memorizing the classification, ask yourself—can the venous outflow handle the flow (dural sinus vs cortical vein) & does it look like it is overwhelmed (venous ectasia)?
This will intuitively lead you to the classification system w/o having to memorize a thing!
This will intuitively lead you to the classification system w/o having to memorize a thing!
14/Cognard classification defines dAVFs by the type of venous drainage—and it progresses just how I described.
If flow can go forward, it can--if not, it goes retrograde & risk of bleeding goes up by how badly the retrograde flow affects cortical veins.
If flow can go forward, it can--if not, it goes retrograde & risk of bleeding goes up by how badly the retrograde flow affects cortical veins.

December 19, 2024 at 2:25 PM
14/Cognard classification defines dAVFs by the type of venous drainage—and it progresses just how I described.
If flow can go forward, it can--if not, it goes retrograde & risk of bleeding goes up by how badly the retrograde flow affects cortical veins.
If flow can go forward, it can--if not, it goes retrograde & risk of bleeding goes up by how badly the retrograde flow affects cortical veins.
13/Cortical reflux is the dividing line whether a fistula will have benign course or is likely to bleed—bc cortical veins can’t handle flow like dural sinuses & are thus more likely to bleed.

December 19, 2024 at 2:25 PM
13/Cortical reflux is the dividing line whether a fistula will have benign course or is likely to bleed—bc cortical veins can’t handle flow like dural sinuses & are thus more likely to bleed.
12/If fistula flow goes retrograde into the spinal veins, these are clearly not ready for high flow from a brain AVF & are quickly overwhelmed.
If pressure is high in veins draining the cord, the cord can’t drain & you get venous HTN like a regular spinal AVF.
If pressure is high in veins draining the cord, the cord can’t drain & you get venous HTN like a regular spinal AVF.

December 19, 2024 at 2:25 PM
12/If fistula flow goes retrograde into the spinal veins, these are clearly not ready for high flow from a brain AVF & are quickly overwhelmed.
If pressure is high in veins draining the cord, the cord can’t drain & you get venous HTN like a regular spinal AVF.
If pressure is high in veins draining the cord, the cord can’t drain & you get venous HTN like a regular spinal AVF.
11/When the cortical veins of a dAVF become dilated, it’s a sign that the flow is too much for them & they are trying to remodel to accommodate.
This is a sign that they are failing & increases the risk that they’ll bleed.
This is a sign that they are failing & increases the risk that they’ll bleed.

December 19, 2024 at 2:25 PM
11/When the cortical veins of a dAVF become dilated, it’s a sign that the flow is too much for them & they are trying to remodel to accommodate.
This is a sign that they are failing & increases the risk that they’ll bleed.
This is a sign that they are failing & increases the risk that they’ll bleed.
10/Unlike dural sinuses, cortical veins are not equipped to handle this flow.
It’s like you put the weight of the earth on a puny human instead of Atlas. Flow is too much for cortical veins to handle and they are more likely to bleed.

December 19, 2024 at 2:25 PM
10/Unlike dural sinuses, cortical veins are not equipped to handle this flow.
It’s like you put the weight of the earth on a puny human instead of Atlas. Flow is too much for cortical veins to handle and they are more likely to bleed.