



F. Perry Wilson, MD
@fperrywilson.bsky.social
Director, Clinical and Translational Research Accelerator @Yale. Columnist @medscape.
How Medicine Works and When It Doesn't in bookstores now!
How Medicine Works and When It Doesn't in bookstores now!
I break down the full paper, the physiology of the rebound, and what this means for the future of obesity medicine @medscape: buff.ly/4jvQhAO
/🧵
/🧵

November 24, 2025 at 11:27 PM
I break down the full paper, the physiology of the rebound, and what this means for the future of obesity medicine @medscape: buff.ly/4jvQhAO
/🧵
/🧵
he hard truth: For the vast majority, stopping GLP-1s means an eventual return to baseline.
We are in a new paradigm of chronic weight management. "Miracle" implies a cure. This is a treatment. And right now, it looks like it might be a forever one.
We are in a new paradigm of chronic weight management. "Miracle" implies a cure. This is a treatment. And right now, it looks like it might be a forever one.
November 24, 2025 at 11:27 PM
he hard truth: For the vast majority, stopping GLP-1s means an eventual return to baseline.
We are in a new paradigm of chronic weight management. "Miracle" implies a cure. This is a treatment. And right now, it looks like it might be a forever one.
We are in a new paradigm of chronic weight management. "Miracle" implies a cure. This is a treatment. And right now, it looks like it might be a forever one.
But there were also weight independent effects. Here you see the increase in systolic blood pressure after stopping the drug. It goes up even among people who are able to keep the weight off.

November 24, 2025 at 11:27 PM
But there were also weight independent effects. Here you see the increase in systolic blood pressure after stopping the drug. It goes up even among people who are able to keep the weight off.
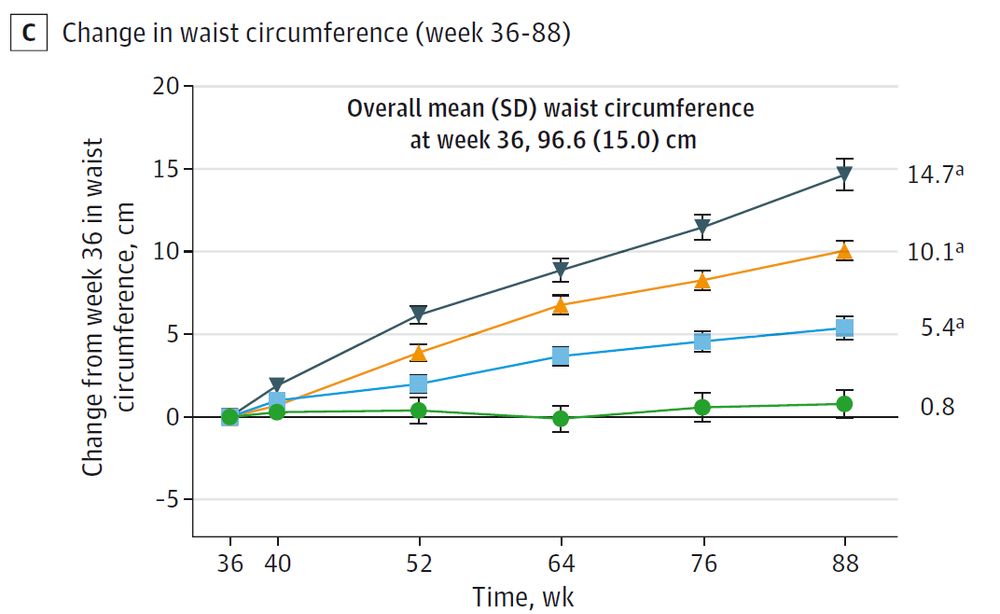
With the regain in weight came increases in weight-associated factors, like waist circumference.
November 24, 2025 at 11:27 PM
With the regain in weight came increases in weight-associated factors, like waist circumference.
People who lost more weight ON the drug were more likely to keep it off. That might reflect something like "commitment to weight loss" which is hard to measure. But you don't know how much people will lose before treatment starts.

November 24, 2025 at 11:27 PM
People who lost more weight ON the drug were more likely to keep it off. That might reflect something like "commitment to weight loss" which is hard to measure. But you don't know how much people will lose before treatment starts.
What predicts who will regain weight? Let's look at the baseline data.
Was it age? BMI? Insulin levels?
Answer: None of them. Nothing at baseline predicted who would be able to keep the weight off. We are essentially flying blind.
Was it age? BMI? Insulin levels?
Answer: None of them. Nothing at baseline predicted who would be able to keep the weight off. We are essentially flying blind.

November 24, 2025 at 11:27 PM
What predicts who will regain weight? Let's look at the baseline data.
Was it age? BMI? Insulin levels?
Answer: None of them. Nothing at baseline predicted who would be able to keep the weight off. We are essentially flying blind.
Was it age? BMI? Insulin levels?
Answer: None of them. Nothing at baseline predicted who would be able to keep the weight off. We are essentially flying blind.
We might hope these drugs "reset" our body weight thermostat to a new, lower baseline.
This data confirms they do NOT work that way. The thermostat is still set where it always was. Once the drug leaves your system, biology fights to get you back to your starting weight.
This data confirms they do NOT work that way. The thermostat is still set where it always was. Once the drug leaves your system, biology fights to get you back to your starting weight.
November 24, 2025 at 11:27 PM
We might hope these drugs "reset" our body weight thermostat to a new, lower baseline.
This data confirms they do NOT work that way. The thermostat is still set where it always was. Once the drug leaves your system, biology fights to get you back to your starting weight.
This data confirms they do NOT work that way. The thermostat is still set where it always was. Once the drug leaves your system, biology fights to get you back to your starting weight.
We finally have a detailed look at the people who stopped.
This waterfall plot is dramatic. Each bar is one person.
82.5% of people regained significant weight. Almost NO ONE could maintain the loss without the drug.
This waterfall plot is dramatic. Each bar is one person.
82.5% of people regained significant weight. Almost NO ONE could maintain the loss without the drug.

November 24, 2025 at 11:27 PM
We finally have a detailed look at the people who stopped.
This waterfall plot is dramatic. Each bar is one person.
82.5% of people regained significant weight. Almost NO ONE could maintain the loss without the drug.
This waterfall plot is dramatic. Each bar is one person.
82.5% of people regained significant weight. Almost NO ONE could maintain the loss without the drug.
This comes from a new post-hoc analysis of the SURMOUNT-4 trial.
The setup: Participants took tirzepatide for 36 weeks. They lost ~20% of their body weight.
Then, half were switched to placebo. The other half stayed on the drug.
buff.ly/mCCtwHc
The setup: Participants took tirzepatide for 36 weeks. They lost ~20% of their body weight.
Then, half were switched to placebo. The other half stayed on the drug.
buff.ly/mCCtwHc


November 24, 2025 at 11:27 PM
This comes from a new post-hoc analysis of the SURMOUNT-4 trial.
The setup: Participants took tirzepatide for 36 weeks. They lost ~20% of their body weight.
Then, half were switched to placebo. The other half stayed on the drug.
buff.ly/mCCtwHc
The setup: Participants took tirzepatide for 36 weeks. They lost ~20% of their body weight.
Then, half were switched to placebo. The other half stayed on the drug.
buff.ly/mCCtwHc
But if substitution is real, some of that national trend might not be coincidence. And that makes this study, despite its modest size, an important signal.
More here in my @medscape column this week: buff.ly/pM9bU3k
More here in my @medscape column this week: buff.ly/pM9bU3k
November 19, 2025 at 4:24 PM
But if substitution is real, some of that national trend might not be coincidence. And that makes this study, despite its modest size, an important signal.
More here in my @medscape column this week: buff.ly/pM9bU3k
More here in my @medscape column this week: buff.ly/pM9bU3k
Caveats:
• These were already alcohol and marijuana users. No idea what happens in non-users.
• This was smoked cannabis only.
• Lab behavior ≠ real-world behavior.
Still, it lines up intriguingly with declining alcohol consumption since cannabis decriminalization.
• These were already alcohol and marijuana users. No idea what happens in non-users.
• This was smoked cannabis only.
• Lab behavior ≠ real-world behavior.
Still, it lines up intriguingly with declining alcohol consumption since cannabis decriminalization.
November 19, 2025 at 4:24 PM
Caveats:
• These were already alcohol and marijuana users. No idea what happens in non-users.
• This was smoked cannabis only.
• Lab behavior ≠ real-world behavior.
Still, it lines up intriguingly with declining alcohol consumption since cannabis decriminalization.
• These were already alcohol and marijuana users. No idea what happens in non-users.
• This was smoked cannabis only.
• Lab behavior ≠ real-world behavior.
Still, it lines up intriguingly with declining alcohol consumption since cannabis decriminalization.
This has... implications. If THC reduces alcohol intake in regular dual-users, that smells a lot like harm-reduction logic. Controversial? Sure. But from a public health standpoint, alcohol is unquestionably the more dangerous drug of the two.
November 19, 2025 at 4:24 PM
This has... implications. If THC reduces alcohol intake in regular dual-users, that smells a lot like harm-reduction logic. Controversial? Sure. But from a public health standpoint, alcohol is unquestionably the more dangerous drug of the two.
This is strong support for the substitution hypothesis. People are chasing a subjective state, and THC can partially “fill the slot” that alcohol normally occupies.
November 19, 2025 at 4:24 PM
This is strong support for the substitution hypothesis. People are chasing a subjective state, and THC can partially “fill the slot” that alcohol normally occupies.
But consumption? Completely different story.
Average number of drinks:
• Placebo: ~3
• Low-dose THC: 2.4
• High-dose THC: 2.1
Nice dose-response. Statistically significant. And the direction is reversed from the authors’ original hypothesis.
Average number of drinks:
• Placebo: ~3
• Low-dose THC: 2.4
• High-dose THC: 2.1
Nice dose-response. Statistically significant. And the direction is reversed from the authors’ original hypothesis.

November 19, 2025 at 4:24 PM
But consumption? Completely different story.
Average number of drinks:
• Placebo: ~3
• Low-dose THC: 2.4
• High-dose THC: 2.1
Nice dose-response. Statistically significant. And the direction is reversed from the authors’ original hypothesis.
Average number of drinks:
• Placebo: ~3
• Low-dose THC: 2.4
• High-dose THC: 2.1
Nice dose-response. Statistically significant. And the direction is reversed from the authors’ original hypothesis.
Cravings went up slightly when participants were shown images of their preferred alcohol. But THC didn’t change cravings meaningfully. The craving curves looked the same whether people smoked placebo or high-dose THC.

November 19, 2025 at 4:24 PM
Cravings went up slightly when participants were shown images of their preferred alcohol. But THC didn’t change cravings meaningfully. The craving curves looked the same whether people smoked placebo or high-dose THC.
The hypothesis? Higher THC → more alcohol consumption (the complementarity idea).
The reality: basically the exact opposite.
The reality: basically the exact opposite.
November 19, 2025 at 4:24 PM
The hypothesis? Higher THC → more alcohol consumption (the complementarity idea).
The reality: basically the exact opposite.
The reality: basically the exact opposite.
Then came the fun part: the bar lab.
For two hours, participants could drink up to eight mini drinks. But for every drink they didn’t consume, they earned $3. A tidy little behavioral economics setup.
For two hours, participants could drink up to eight mini drinks. But for every drink they didn’t consume, they earned $3. A tidy little behavioral economics setup.

November 19, 2025 at 4:24 PM
Then came the fun part: the bar lab.
For two hours, participants could drink up to eight mini drinks. But for every drink they didn’t consume, they earned $3. A tidy little behavioral economics setup.
For two hours, participants could drink up to eight mini drinks. But for every drink they didn’t consume, they earned $3. A tidy little behavioral economics setup.
And the THC definitely did something. Participants reported more happiness, more anxiety (classic), and had measurable increases in heart rate. So we know the doses weren’t trivial.


November 19, 2025 at 4:24 PM
And the THC definitely did something. Participants reported more happiness, more anxiety (classic), and had measurable increases in heart rate. So we know the doses weren’t trivial.
They recruited 157 people who regularly use both alcohol and marijuana. Each participant came into the lab on 3 occasions, smoking:
• a placebo joint
• a 3.1% THC joint
• a 7.2% THC joint
(in random order)
• a placebo joint
• a 3.1% THC joint
• a 7.2% THC joint
(in random order)

November 19, 2025 at 4:24 PM
They recruited 157 people who regularly use both alcohol and marijuana. Each participant came into the lab on 3 occasions, smoking:
• a placebo joint
• a 3.1% THC joint
• a 7.2% THC joint
(in random order)
• a placebo joint
• a 3.1% THC joint
• a 7.2% THC joint
(in random order)
The substitution model is especially interesting: even if both drugs show up together in the real world, one might suppress the other when conditions are controlled. But that’s a hard thing to study. Enter Dr. Jane Metrik’s group. buff.ly/nUuJPg5

November 19, 2025 at 4:24 PM
The substitution model is especially interesting: even if both drugs show up together in the real world, one might suppress the other when conditions are controlled. But that’s a hard thing to study. Enter Dr. Jane Metrik’s group. buff.ly/nUuJPg5
Substitution: people are just looking to “feel different,” and any drug that gets them there competes with the others.

November 19, 2025 at 4:24 PM
Substitution: people are just looking to “feel different,” and any drug that gets them there competes with the others.
Phenotype: the same “type” of person tends to use both; the drugs are correlated because people bring their traits with them.

November 19, 2025 at 4:24 PM
Phenotype: the same “type” of person tends to use both; the drugs are correlated because people bring their traits with them.
There are a few possible models in this space.
Complementarity: marijuana makes you more likely to drink; lower inhibitions, more risk-taking, maybe more craving.
Complementarity: marijuana makes you more likely to drink; lower inhibitions, more risk-taking, maybe more craving.

November 19, 2025 at 4:24 PM
There are a few possible models in this space.
Complementarity: marijuana makes you more likely to drink; lower inhibitions, more risk-taking, maybe more craving.
Complementarity: marijuana makes you more likely to drink; lower inhibitions, more risk-taking, maybe more craving.
So how do you get from that to a randomized trial showing that THC suppresses drinking? Classic case of correlation not equaling causation.
November 19, 2025 at 4:24 PM
So how do you get from that to a randomized trial showing that THC suppresses drinking? Classic case of correlation not equaling causation.