




Willy Frick
@willyhfrick.bsky.social
Heart rhythm fellow. Medical educator. ECG enthusiast.
Associate Editor of Dr. Smith's ECG Blog: https://drsmithsecgblog.com
Associate Editor of Dr. Smith's ECG Blog: https://drsmithsecgblog.com
Pinned
Willy Frick
@willyhfrick.bsky.social
· Nov 25

For anyone interested in learning more about angiography, check out my introductory guide!
You’ll find a lot of nice annotated diagrams like this one.
intuitivecardiology.notion.site/angiography
You’ll find a lot of nice annotated diagrams like this one.
intuitivecardiology.notion.site/angiography
Do #EPeeps believe in AVNRT upper common pathway (block)?
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible

October 21, 2025 at 1:43 AM
Do #EPeeps believe in AVNRT upper common pathway (block)?
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible
Arrhythmogenic cardiomyopathy, epicardial access. Pacing from ablator.
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps

October 17, 2025 at 5:09 PM
Arrhythmogenic cardiomyopathy, epicardial access. Pacing from ablator.
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps

June 20, 2025 at 9:55 PM

June 17, 2025 at 4:47 PM
Does the constancy of the PVC coupling interval suggest triggered mechanism?
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social

June 11, 2025 at 3:42 AM
Does the constancy of the PVC coupling interval suggest triggered mechanism?
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social

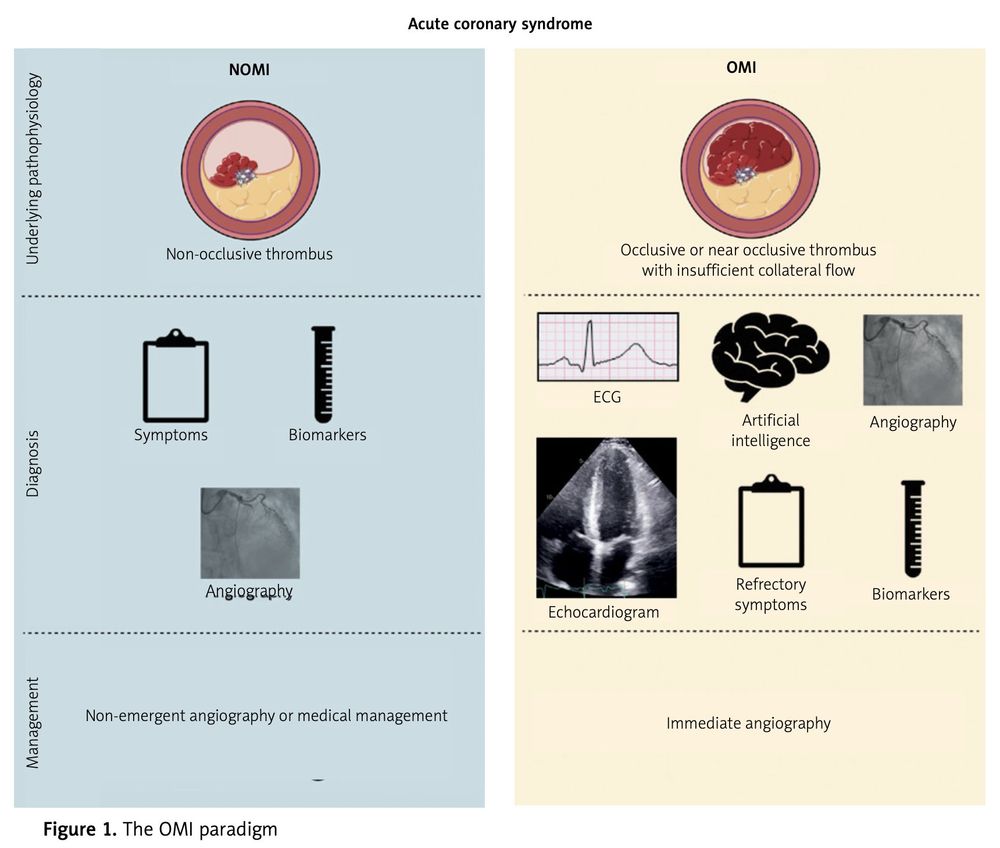
Read our editorial at the link below!
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social
June 3, 2025 at 8:58 PM
Read our editorial at the link below!
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social


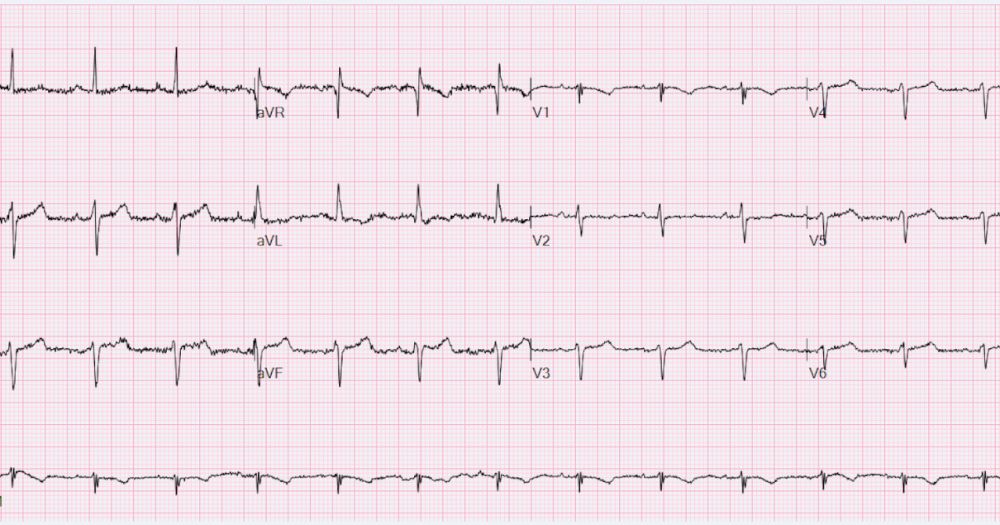
60M with severe ischemic cardiomyopathy, prior inferoposterior OMI.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.

May 14, 2025 at 2:06 PM
60M with severe ischemic cardiomyopathy, prior inferoposterior OMI.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.
I can't figure out an elegant explanation for the intermittent aberrancy.
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps

April 25, 2025 at 10:33 PM
I can't figure out an elegant explanation for the intermittent aberrancy.
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps

April 12, 2025 at 7:15 PM
Reposted by Willy Frick

VT entrainment.
Some of you want to learn it from the beginning.
Some just want the punchline.
Here's a direct link to the climax of the video, with examples of all the possible entrainment locations (isthmus, entrance, exit, bystander, outer loop, etc)
youtu.be/XykkZNLm9bc?...
Some of you want to learn it from the beginning.
Some just want the punchline.
Here's a direct link to the climax of the video, with examples of all the possible entrainment locations (isthmus, entrance, exit, bystander, outer loop, etc)
youtu.be/XykkZNLm9bc?...
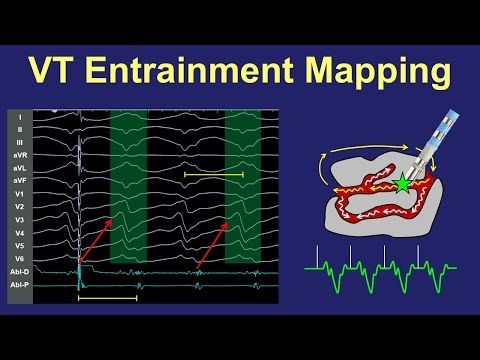
VT Entrainment Mapping of Scar/Reentry VT
YouTube video by Dr. Joshua Cooper - Arrhythmia Education
youtu.be
April 10, 2025 at 9:12 PM
VT entrainment.
Some of you want to learn it from the beginning.
Some just want the punchline.
Here's a direct link to the climax of the video, with examples of all the possible entrainment locations (isthmus, entrance, exit, bystander, outer loop, etc)
youtu.be/XykkZNLm9bc?...
Some of you want to learn it from the beginning.
Some just want the punchline.
Here's a direct link to the climax of the video, with examples of all the possible entrainment locations (isthmus, entrance, exit, bystander, outer loop, etc)
youtu.be/XykkZNLm9bc?...
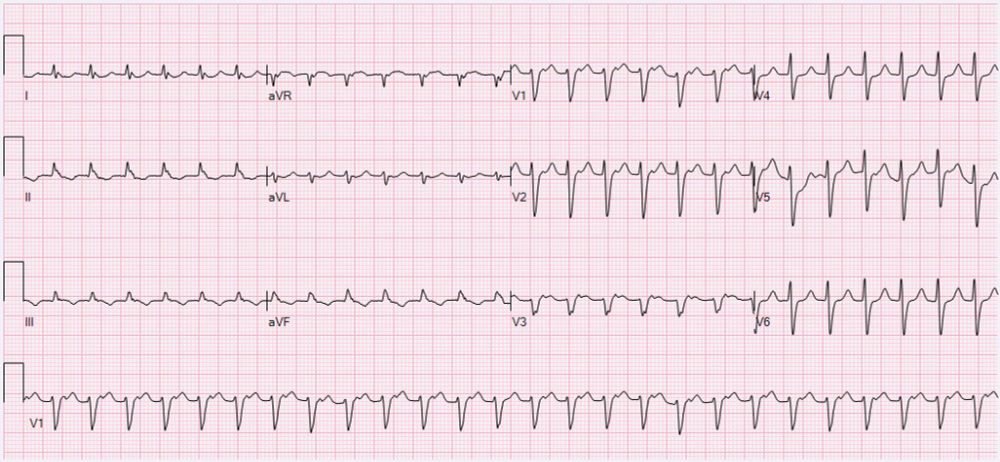
Overhead page code blue. You arrive bedside to find ongoing chest compressions. First pulse check, you see this.
What next?
#cardiosky
What next?
#cardiosky

April 7, 2025 at 2:25 AM
Overhead page code blue. You arrive bedside to find ongoing chest compressions. First pulse check, you see this.
What next?
#cardiosky
What next?
#cardiosky
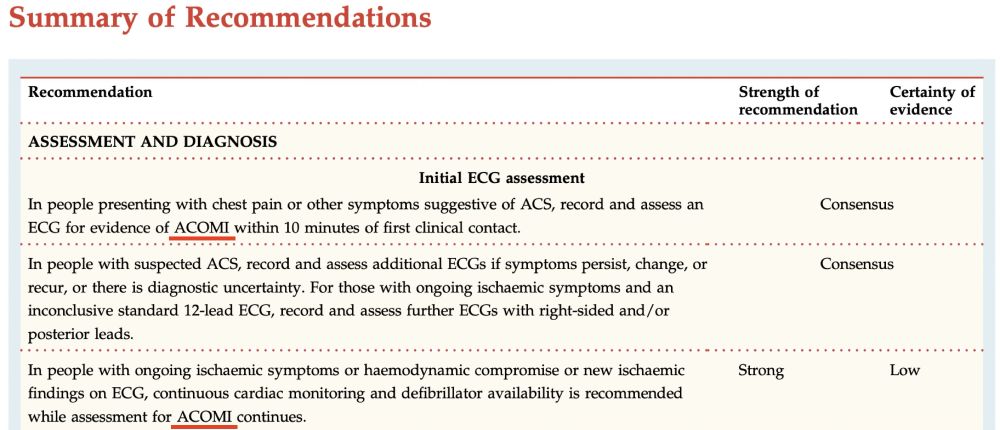
Glad to see the Australian guidelines reflect the data where American guidelines (@accintouch.bsky.social) were stuck in an antiquated era.
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
April 6, 2025 at 1:17 PM
Glad to see the Australian guidelines reflect the data where American guidelines (@accintouch.bsky.social) were stuck in an antiquated era.
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
Fred W. Frick, MD FACP, inducted 2000
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social

April 4, 2025 at 2:21 AM
Fred W. Frick, MD FACP, inducted 2000
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social
Reposted by Willy Frick

New publication for my OMI colleagues @sargsyanz.bsky.social @willyhfrick.bsky.social 💀
bhm.scholasticahq.com/article/1337...
bhm.scholasticahq.com/article/1337...
Posterior Occlusive Myocardial Infarction on Chronic Right Bundle Branch Block | Published in Journal of Brown Hospital Medicine
By Andrew Sanchez, Omar El-Charif. An elderly woman with chronic RBBB presented in shock and was diagnosed with posterior myocardial infarction
bhm.scholasticahq.com
April 1, 2025 at 1:11 PM
New publication for my OMI colleagues @sargsyanz.bsky.social @willyhfrick.bsky.social 💀
bhm.scholasticahq.com/article/1337...
bhm.scholasticahq.com/article/1337...

April 1, 2025 at 12:58 AM
Reposted by Willy Frick

"Your symptoms are critically important to me… If you have ANY chest discomfort [or whatever symptom the patient was experiencing] I need to know immediately. Please tell me or tell your nurse, because that would be an emergency."
hqmeded-ecg.blogspot.com/2025/03/ever...
@willyhfrick.bsky.social
hqmeded-ecg.blogspot.com/2025/03/ever...
@willyhfrick.bsky.social

Everyone sees ST depression, but what does it mean?
Emergency cardiac care, cardiology, EKGs, ECGs, electrocardiography, echocardiography, dysrhythmias, arrhythmias, STEMI, NonSTEMI, NSTEMI, cardiology
hqmeded-ecg.blogspot.com
March 30, 2025 at 12:58 PM
"Your symptoms are critically important to me… If you have ANY chest discomfort [or whatever symptom the patient was experiencing] I need to know immediately. Please tell me or tell your nurse, because that would be an emergency."
hqmeded-ecg.blogspot.com/2025/03/ever...
@willyhfrick.bsky.social
hqmeded-ecg.blogspot.com/2025/03/ever...
@willyhfrick.bsky.social
I'm delving into new territory here with narrated videos. Please tell me how I can improve!
#ECGsky #medsky #cardiosky
#ECGsky #medsky #cardiosky
Can you localize the culprit lesion on angiogram without taking ECG findings into account?
Emergency cardiac care, cardiology, EKGs, ECGs, electrocardiography, echocardiography, dysrhythmias, arrhythmias, STEMI, NonSTEMI, NSTEMI, cardiology
hqmeded-ecg.blogspot.com
March 25, 2025 at 2:45 PM
I'm delving into new territory here with narrated videos. Please tell me how I can improve!
#ECGsky #medsky #cardiosky
#ECGsky #medsky #cardiosky

Reposted by Willy Frick
🚨 OMG, I actually just sat down and did my video narration of my VT entrainment talk (!!!)
I'm converting to MP4 video right now.
Might upload to YouTube soon, or I might go to bed and upload within the next day.
But holy cow, it was a big effort and I'm so glad to get it done!!!!
I'm converting to MP4 video right now.
Might upload to YouTube soon, or I might go to bed and upload within the next day.
But holy cow, it was a big effort and I'm so glad to get it done!!!!

March 16, 2025 at 7:16 AM
🚨 OMG, I actually just sat down and did my video narration of my VT entrainment talk (!!!)
I'm converting to MP4 video right now.
Might upload to YouTube soon, or I might go to bed and upload within the next day.
But holy cow, it was a big effort and I'm so glad to get it done!!!!
I'm converting to MP4 video right now.
Might upload to YouTube soon, or I might go to bed and upload within the next day.
But holy cow, it was a big effort and I'm so glad to get it done!!!!
New update just dropped in the coronary anomalies section!

March 15, 2025 at 5:41 PM
New update just dropped in the coronary anomalies section!
Recent emotional case that made a big impact on me. I don’t have all the answers. Tell me what you think. Lit review at the bottom
#ECGsky #medsky #cardiosky
hqmeded-ecg.blogspot.com/2025/03/pati...
#ECGsky #medsky #cardiosky
hqmeded-ecg.blogspot.com/2025/03/pati...

Patient is informed of her husband's death: is it OMI or it stress cardiomyopathy?
Emergency cardiac care, cardiology, EKGs, ECGs, electrocardiography, echocardiography, dysrhythmias, arrhythmias, STEMI, NonSTEMI, NSTEMI, cardiology
hqmeded-ecg.blogspot.com
March 8, 2025 at 3:04 PM
Recent emotional case that made a big impact on me. I don’t have all the answers. Tell me what you think. Lit review at the bottom
#ECGsky #medsky #cardiosky
hqmeded-ecg.blogspot.com/2025/03/pati...
#ECGsky #medsky #cardiosky
hqmeded-ecg.blogspot.com/2025/03/pati...
