


Johannes Enevoldsen
@johsenevoldsen.bsky.social
1.1K followers
290 following
100 posts
MD, PhD. Currently in Nephrology. Interested in health, statistics and scientific programming (R and Julia)
Posts
Media
Videos
Starter Packs
Pinned
Reposted by Johannes Enevoldsen


Reposted by Johannes Enevoldsen

Reposted by Johannes Enevoldsen


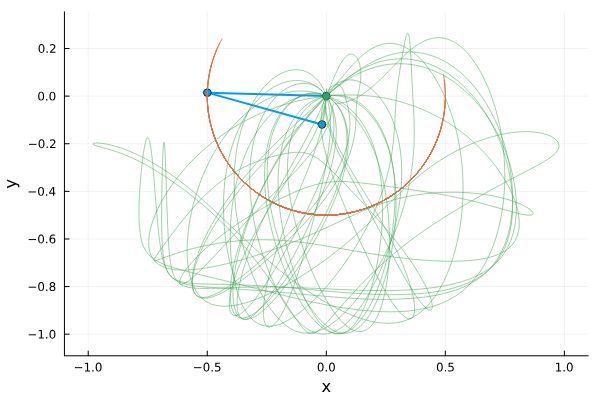
My cardiac arrhythmia simulation now also simulates how a reentrant loop can be terminated by increasing refractory time as suggested by @empoisonpharmd.bsky.social
Direct link to the updated part:
jenevoldsen.com/posts/excita...
Direct link to the updated part:
jenevoldsen.com/posts/excita...
Reposted by Johannes Enevoldsen


Lactate infusion enhances cardiac output and peripheral perfusion in ischemic cardiogenic shock without affecting heart rate or systemic blood pressure, finds a study published in Critical Care.
#MedSky
#MedSky
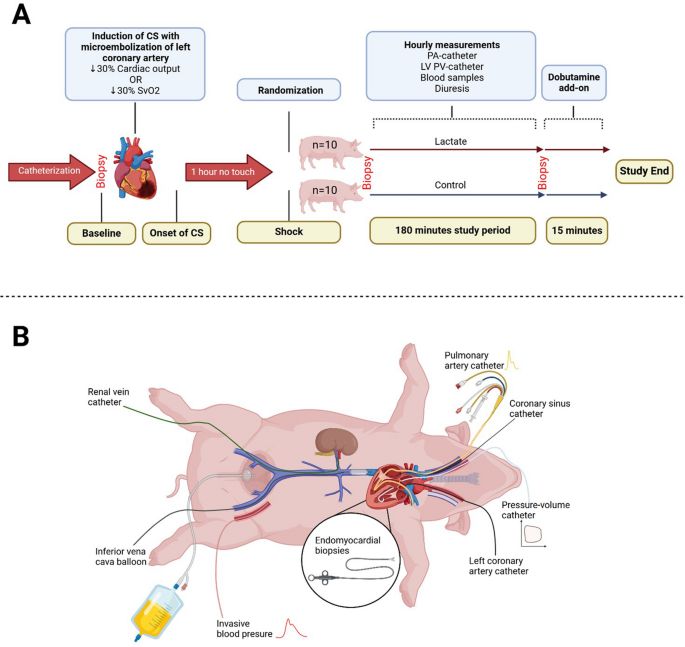
Lactate infusion improves cardiac function in a porcine model of ischemic cardiogenic shock
Critical Care
bit.ly
Reposted by Johannes Enevoldsen

Reposted by Johannes Enevoldsen

I wrote a short interactive article👆
It uses simulations to demonstrate how different cardiac arrhythmias can develop.
Try it out! (It has defibrillators ⚡️)
jenevoldsen.com/posts/excitable-cells
#medsky #cardiosky #cccsky #emimcc
It uses simulations to demonstrate how different cardiac arrhythmias can develop.
Try it out! (It has defibrillators ⚡️)
jenevoldsen.com/posts/excitable-cells
#medsky #cardiosky #cccsky #emimcc