




Christopher Russell, MD, MS (he/his/him)
@cjrussellmd.bsky.social
Associate Professor, Pediatric Hospitalist, Stanford Medicine Children’s Health. Physician-scientist & clinical researcher studying children with medical complexity. Views my own. 🏳️🌈
More at https://med.stanford.edu/profiles/314127
More at https://med.stanford.edu/profiles/314127
Pinned

SGIM and NAPCRG File Lawsuit Against HHS Over Halt to AHRQ Grantmaking - SGIM
The Society of General Internal Medicine (SGIM) and the North American Primary Care Research Group (NAPCRG) have filed a lawsuit against the Department of Health and Human Services (HHS) for halting a...
www.sgim.org
🚨🚨This directly affects me, as I may not get year 5 of my award that was set to be renewed 8/1. Spent 4 years of #AHRQ funding to collect data on children with #tracheostomy. If not resolved by 9/30, I may not have the funding to analyze the data. www.sgim.org/news/sgim-an...
Reposted by Christopher Russell, MD, MS (he/his/him)
🚨🚨This directly affects me, as I may not get year 5 of my award that was set to be renewed 8/1. Spent 4 years of #AHRQ funding to collect data on children with #tracheostomy. If not resolved by 9/30, I may not have the funding to analyze the data. www.sgim.org/news/sgim-an...
SGIM and NAPCRG File Lawsuit Against HHS Over Halt to AHRQ Grantmaking - SGIM
The Society of General Internal Medicine (SGIM) and the North American Primary Care Research Group (NAPCRG) have filed a lawsuit against the Department of Health and Human Services (HHS) for halting a...
www.sgim.org
September 7, 2025 at 2:23 AM
🚨🚨This directly affects me, as I may not get year 5 of my award that was set to be renewed 8/1. Spent 4 years of #AHRQ funding to collect data on children with #tracheostomy. If not resolved by 9/30, I may not have the funding to analyze the data. www.sgim.org/news/sgim-an...
🚨🚨This directly affects me, as I may not get year 5 of my award that was set to be renewed 8/1. Spent 4 years of #AHRQ funding to collect data on children with #tracheostomy. If not resolved by 9/30, I may not have the funding to analyze the data. www.sgim.org/news/sgim-an...
SGIM and NAPCRG File Lawsuit Against HHS Over Halt to AHRQ Grantmaking - SGIM
The Society of General Internal Medicine (SGIM) and the North American Primary Care Research Group (NAPCRG) have filed a lawsuit against the Department of Health and Human Services (HHS) for halting a...
www.sgim.org
September 7, 2025 at 2:23 AM
🚨🚨This directly affects me, as I may not get year 5 of my award that was set to be renewed 8/1. Spent 4 years of #AHRQ funding to collect data on children with #tracheostomy. If not resolved by 9/30, I may not have the funding to analyze the data. www.sgim.org/news/sgim-an...
Reposted by Christopher Russell, MD, MS (he/his/him)

I'm Dr. Annie Andrews. I’m a pediatrician, not a politician. But either way I know how to handle people who are full of sh*t.
Today I am announcing my campaign for US Senate to replace Lindsey Graham. Share this if you're with me.
www.youtube.com/watch?v=J8wM...
Today I am announcing my campaign for US Senate to replace Lindsey Graham. Share this if you're with me.
www.youtube.com/watch?v=J8wM...

Annie Andrews Launch Video: "Unafraid"
YouTube video by Annie Andrews
www.youtube.com
May 29, 2025 at 11:50 AM
I'm Dr. Annie Andrews. I’m a pediatrician, not a politician. But either way I know how to handle people who are full of sh*t.
Today I am announcing my campaign for US Senate to replace Lindsey Graham. Share this if you're with me.
www.youtube.com/watch?v=J8wM...
Today I am announcing my campaign for US Senate to replace Lindsey Graham. Share this if you're with me.
www.youtube.com/watch?v=J8wM...
Reposted by Christopher Russell, MD, MS (he/his/him)

Stanford’s president and provost release a statement supporting Harvard. stanforddaily.com/2025/04/15/l...

Stanford president and provost back Harvard in funding fight
The president and provost said Harvard’s rejection of government demands was “rooted in the American tradition of liberty.”
stanforddaily.com
April 15, 2025 at 1:59 PM
Stanford’s president and provost release a statement supporting Harvard. stanforddaily.com/2025/04/15/l...
Reposted by Christopher Russell, MD, MS (he/his/him)

Harvard has set an example for other higher-ed institutions - rejecting an unlawful and ham-handed attempt to stifle academic freedom, while taking steps to make sure students can benefit from an environment of intellectual inquiry, rigorous debate and mutual respect. Let’s hope others follow suit.
April 15, 2025 at 3:52 AM
Harvard has set an example for other higher-ed institutions - rejecting an unlawful and ham-handed attempt to stifle academic freedom, while taking steps to make sure students can benefit from an environment of intellectual inquiry, rigorous debate and mutual respect. Let’s hope others follow suit.
The Promise of American Higher Education: www.harvard.edu/president/ne...
April 15, 2025 at 12:56 AM
The Promise of American Higher Education: www.harvard.edu/president/ne...
Proud of my alma mater: “We have informed the administration through our legal counsel that we will not accept their proposed agreement. The University will not surrender its independence or relinquish its constitutional rights.”

Harvard rejects Trump administration’s demands with federal funding at risk
The university’s response comes after the government announced a federal review of nearly $9 billion in funding to Harvard and its affiliates.
wapo.st
April 15, 2025 at 12:54 AM
Proud of my alma mater: “We have informed the administration through our legal counsel that we will not accept their proposed agreement. The University will not surrender its independence or relinquish its constitutional rights.”
Reposted by Christopher Russell, MD, MS (he/his/him)

The NIH grant that has supported 38 years of training the best pediatrician-scientists in the country (I’m a proud former recipient) was cancelled. It was just approved for a 5 year renewal. The PSDP has supported the careers of many NIH-funded pediatrician-scientists and thought leaders
March 25, 2025 at 2:53 PM
The NIH grant that has supported 38 years of training the best pediatrician-scientists in the country (I’m a proud former recipient) was cancelled. It was just approved for a 5 year renewal. The PSDP has supported the careers of many NIH-funded pediatrician-scientists and thought leaders
Reposted by Christopher Russell, MD, MS (he/his/him)

This censorship of science is SHAMEFUL. www.nature.com/articles/d41...

Exclusive: NIH to terminate hundreds of active research grants
Studies that touch on LGBT+ health, gender identity and DEI in the biomedical workforce could be terminated, according to documents obtained by Nature.
www.nature.com
March 6, 2025 at 2:37 PM
This censorship of science is SHAMEFUL. www.nature.com/articles/d41...
Reposted by Christopher Russell, MD, MS (he/his/him)

Preliminary injunction in nationwide indirect cost rate case.
This means that the judge found that the plaintiffs (AAMC, et al.) are likely to win on the merits when the ruling is finalized.
www.statnews.com/2025/03/05/n...
This means that the judge found that the plaintiffs (AAMC, et al.) are likely to win on the merits when the ruling is finalized.
www.statnews.com/2025/03/05/n...

Judge issues preliminary injunction blocking Trump cuts to NIH research overhead payments
A federal judge issued a nationwide preliminary injunction blocking the Trump administration from slashing NIH payments for research overhead
www.statnews.com
March 5, 2025 at 9:08 PM
Preliminary injunction in nationwide indirect cost rate case.
This means that the judge found that the plaintiffs (AAMC, et al.) are likely to win on the merits when the ruling is finalized.
www.statnews.com/2025/03/05/n...
This means that the judge found that the plaintiffs (AAMC, et al.) are likely to win on the merits when the ruling is finalized.
www.statnews.com/2025/03/05/n...
Reposted by Christopher Russell, MD, MS (he/his/him)

The University of Pittsburgh confirmed Friday that there would be no new Ph.D. offers of admission while Pitt works to understand how reduced federal aid could impact the institution.

The University of Pittsburgh pauses its Ph.D. admissions process amid research funding uncertainty
A spokesperson for the University told WESA Friday that the school has "temporarily paused additional Ph.D. offers of admission," while Pitt works to understand how proposed federal funding cuts could...
www.wesa.fm
February 21, 2025 at 9:56 PM
The University of Pittsburgh confirmed Friday that there would be no new Ph.D. offers of admission while Pitt works to understand how reduced federal aid could impact the institution.
Reposted by Christopher Russell, MD, MS (he/his/him)

This is a five-alarm fire 🔥 for US science 🧪.
(We keep saying that, but it keeps being true 😭.)
Trump and Musk are blocking *ALL* NIH grants ‼️ by "exploiting a loophole in the process"—stopping study sections & council meetings.
Every biomedical researcher in the country should be screaming. 1/
(We keep saying that, but it keeps being true 😭.)
Trump and Musk are blocking *ALL* NIH grants ‼️ by "exploiting a loophole in the process"—stopping study sections & council meetings.
Every biomedical researcher in the country should be screaming. 1/

NEW: The Trump administration is exploiting a loophole to keep funding frozen at the NIH - a move that some legal scholars say is illegal.
Federal Register notices are blocked, so no grant-review sessions can be scheduled.
All the gritty details here, and a short 🧵:
www.nature.com/articles/d41...
Federal Register notices are blocked, so no grant-review sessions can be scheduled.
All the gritty details here, and a short 🧵:
www.nature.com/articles/d41...

Revealed: NIH research grants still frozen despite lawsuits challenging Trump order
The Trump administration is exploiting a loophole to keep a funding freeze in place, leaving researchers in limbo.
www.nature.com
February 21, 2025 at 4:37 AM
This is a five-alarm fire 🔥 for US science 🧪.
(We keep saying that, but it keeps being true 😭.)
Trump and Musk are blocking *ALL* NIH grants ‼️ by "exploiting a loophole in the process"—stopping study sections & council meetings.
Every biomedical researcher in the country should be screaming. 1/
(We keep saying that, but it keeps being true 😭.)
Trump and Musk are blocking *ALL* NIH grants ‼️ by "exploiting a loophole in the process"—stopping study sections & council meetings.
Every biomedical researcher in the country should be screaming. 1/
Wonderful to collaborate with @lkelley-quon.bsky.social!

Thank you @wordinblacknews.bsky.social for highlighting our @jama.com paper demonstrating The Unequal Weight of a Drug Test. @cjrussellmd.bsky.social @iasatusc.bsky.social @keckmedicineusc.bsky.social

The Unequal Weight of a Drug Test
At trauma centers, youth of color are more likely to be tested for substances. With overdoses rising, why aren’t all kids tested equitably?
wordinblack.com
February 13, 2025 at 4:55 PM
Wonderful to collaborate with @lkelley-quon.bsky.social!
Reposted by Christopher Russell, MD, MS (he/his/him)

How Capping NIH Indirect Costs at 15% Hurts Science, Jobs, and Public Health
1/ The new cap to indirect costs at 15% on NIH grants may sound like a way to cut wasteful spending. In reality, it would devastate biomedical research, slow medical breakthroughs, and cost jobs.
Y'all know I love a good 🧵
1/ The new cap to indirect costs at 15% on NIH grants may sound like a way to cut wasteful spending. In reality, it would devastate biomedical research, slow medical breakthroughs, and cost jobs.
Y'all know I love a good 🧵
February 9, 2025 at 1:03 AM
How Capping NIH Indirect Costs at 15% Hurts Science, Jobs, and Public Health
1/ The new cap to indirect costs at 15% on NIH grants may sound like a way to cut wasteful spending. In reality, it would devastate biomedical research, slow medical breakthroughs, and cost jobs.
Y'all know I love a good 🧵
1/ The new cap to indirect costs at 15% on NIH grants may sound like a way to cut wasteful spending. In reality, it would devastate biomedical research, slow medical breakthroughs, and cost jobs.
Y'all know I love a good 🧵
Reposted by Christopher Russell, MD, MS (he/his/him)

1. Today the NIH director issued a new directive slashing overhead rates to 15%.
I want to provide some context on what that means and why it matters.
grants.nih.gov/grants/guide...
I want to provide some context on what that means and why it matters.
grants.nih.gov/grants/guide...
NOT-OD-25-068: Supplemental Guidance to the 2024 NIH Grants Policy Statement: Indirect Cost Rates
NIH Funding Opportunities and Notices in the NIH Guide for Grants and Contracts: Supplemental Guidance to the 2024 NIH Grants Policy Statement: Indirect Cost Rates NOT-OD-25-068. OD
grants.nih.gov
February 8, 2025 at 12:18 AM
1. Today the NIH director issued a new directive slashing overhead rates to 15%.
I want to provide some context on what that means and why it matters.
grants.nih.gov/grants/guide...
I want to provide some context on what that means and why it matters.
grants.nih.gov/grants/guide...
Reposted by Christopher Russell, MD, MS (he/his/him)

“This is a blatant attempt to gut the universities and health research that have saved so many lives and given economic opportunity to so many people.” @iwashyna.bsky.social on impact of new NIh order to cut research indirect costs. www.statnews.com/2025/02/07/n...

NIH plans to slash support for indirect research costs, sending shockwaves through science
The NIH said Friday night that it would slash support for indirect costs on all existing and future grants to 15%
www.statnews.com
February 8, 2025 at 1:35 AM
“This is a blatant attempt to gut the universities and health research that have saved so many lives and given economic opportunity to so many people.” @iwashyna.bsky.social on impact of new NIh order to cut research indirect costs. www.statnews.com/2025/02/07/n...
🚨 🚨

The NIH capping the indirect cost rate (IDC) for grants at 15% can best be described as a direct assault on Universities. It’s such a bureaucratic, innocuous sounding thing that actually means that research universities will be kneecapped. Thousands of employees across the US will lose their jobs.
February 8, 2025 at 1:39 AM
🚨 🚨
Reposted by Christopher Russell, MD, MS (he/his/him)

Withdrawal of funding mid-trial is a serious violation of research ethics and implicates all of us who engage in clinical research. Ethical review boards around the world will have to re-evaluate allowing US-funded projects. The balance between harm-benefit is complexly upended.
"The trial was shutting down, a nurse told her. The device, a silicone ring inserted into her vagina, needed to be removed right away." jesus christ www.nytimes.com/2025/02/06/h...

Dozens of Clinical Trials Have Been Frozen in Response to Trump’s USAID Order
The stop-work order on U.S.A.I.D.-funded research has left thousands of people with experimental drugs and devices in their bodies, with no access to monitoring or care.
www.nytimes.com
February 7, 2025 at 3:28 AM
Withdrawal of funding mid-trial is a serious violation of research ethics and implicates all of us who engage in clinical research. Ethical review boards around the world will have to re-evaluate allowing US-funded projects. The balance between harm-benefit is complexly upended.
Reposted by Christopher Russell, MD, MS (he/his/him)

BREAKING NEWS: CDC orders mass retraction and revision of submitted research across all science and medicine journals. Banned terms must be scrubbed.
Goes beyond MMWR +other CDC pubs. Applies to research already submitted to top medical journals.
Take a look.
open.substack.com/pub/insideme...
Goes beyond MMWR +other CDC pubs. Applies to research already submitted to top medical journals.
Take a look.
open.substack.com/pub/insideme...
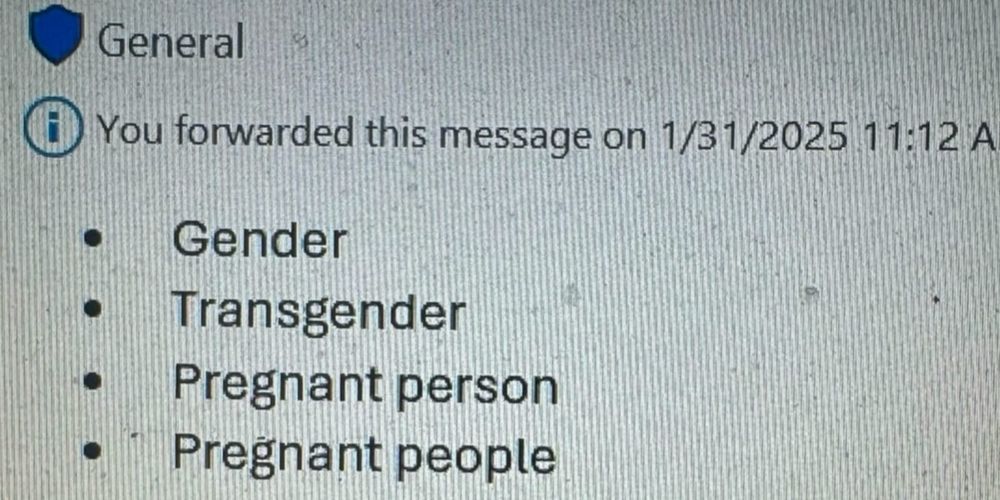
BREAKING NEWS: CDC orders mass retraction and revision of submitted research across all science and medicine journals. Banned terms must be scrubbed.
Any unpublished manuscript mentioning certain topics, including gender and "LGBT," must be pulled or revised.
open.substack.com
February 1, 2025 at 9:20 PM
BREAKING NEWS: CDC orders mass retraction and revision of submitted research across all science and medicine journals. Banned terms must be scrubbed.
Goes beyond MMWR +other CDC pubs. Applies to research already submitted to top medical journals.
Take a look.
open.substack.com/pub/insideme...
Goes beyond MMWR +other CDC pubs. Applies to research already submitted to top medical journals.
Take a look.
open.substack.com/pub/insideme...
Reposted by Christopher Russell, MD, MS (he/his/him)

thinking this morning about how the NIH's definition of diversity also includes uplifting struggling Americans of all races and genders (formerly homeless, on WIC, foster kids, first-gen students, rural Americans, etc)

January 29, 2025 at 4:23 PM
thinking this morning about how the NIH's definition of diversity also includes uplifting struggling Americans of all races and genders (formerly homeless, on WIC, foster kids, first-gen students, rural Americans, etc)
“The White House budget office is ordering a pause to all grants and loans disbursed by the federal government…” including all research grants! 🚨 🚨

White House pauses all federal grants, sparking confusion
The Trump administration has put a hold on all federal financial grants and loans, affecting tens of billions of dollars in payments.
www.washingtonpost.com
January 28, 2025 at 3:09 AM
“The White House budget office is ordering a pause to all grants and loans disbursed by the federal government…” including all research grants! 🚨 🚨
Reposted by Christopher Russell, MD, MS (he/his/him)
The NIH diversity supplement pages have all been pulled down. What is a diversity supplement and why should the public care? A diversity supplement is funding to help diversify the research workforce. You may be wondering, “so what?”. Let me explain. www.nigms.nih.gov/Pages/PageNo...
National Institute of General Medical Sciences
NIGMS supports basic research to understand biological processes and lay the foundation for advances in disease diagnosis, treatment, and prevention.
www.nigms.nih.gov
January 25, 2025 at 3:59 PM
The NIH diversity supplement pages have all been pulled down. What is a diversity supplement and why should the public care? A diversity supplement is funding to help diversify the research workforce. You may be wondering, “so what?”. Let me explain. www.nigms.nih.gov/Pages/PageNo...
Reposted by Christopher Russell, MD, MS (he/his/him)
"Health disparities research" is a field of study where researchers look at how things like race, ethnicity, gender, socioeconomic status can influence health outcomes. Now any gov't website about this says "page not found".
This is a dystopia that I did not imagine that we'd be living through.
This is a dystopia that I did not imagine that we'd be living through.

January 25, 2025 at 9:03 PM
"Health disparities research" is a field of study where researchers look at how things like race, ethnicity, gender, socioeconomic status can influence health outcomes. Now any gov't website about this says "page not found".
This is a dystopia that I did not imagine that we'd be living through.
This is a dystopia that I did not imagine that we'd be living through.