



Anil Makam
@anilmakam.bsky.social
UCSF Hospital Medicine Physician Scientist at SFGH. Think about evidence, clinical medicine, outcomes, health services, policy. https://hopelab.ucsf.edu/people/anil-makam-md
Pinned
Anil Makam
@anilmakam.bsky.social
· Apr 23
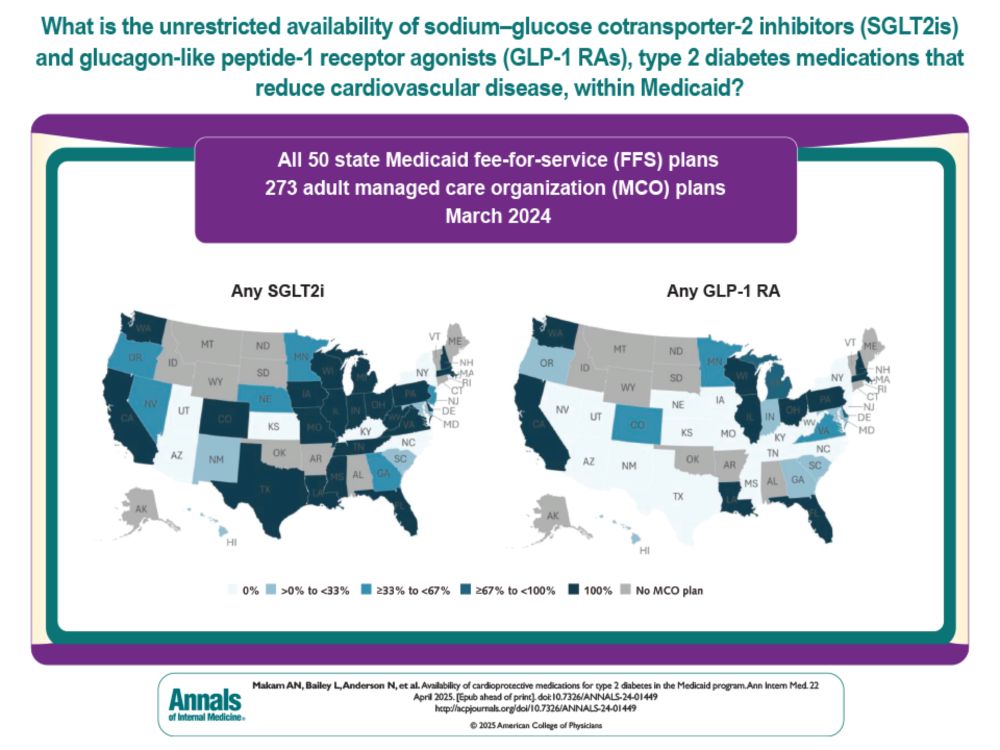
Availability of Cardioprotective Medications for Type 2 Diabetes in the Medicaid Program | Annals of Internal Medicine
Background: Sodium–glucose cotransporter-2 inhibitors (SGLT2is) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are the only type 2 diabetes medications that reduce cardiovascular disease an...
www.acpjournals.org
🚨New Study in Annals🚨
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
Reposted by Anil Makam

A meta-analysis of 5 contemporary trials found no improvement in outcomes with beta blocker therapy after myocardial infarction with normal EF (≥50%)
November 21, 2025 at 4:12 PM
A meta-analysis of 5 contemporary trials found no improvement in outcomes with beta blocker therapy after myocardial infarction with normal EF (≥50%)
Reposted by Anil Makam
Conservative dialysis strategy shows promise for AKI-D
The LIBERATE-D trial found that this approach led to better renal recovery at discharge vs thrice-weekly dialysis (64% vs 50%)
Although adjusted CIs were nonsignificant and deaths were numerically higher
The LIBERATE-D trial found that this approach led to better renal recovery at discharge vs thrice-weekly dialysis (64% vs 50%)
Although adjusted CIs were nonsignificant and deaths were numerically higher
November 20, 2025 at 8:14 PM
Conservative dialysis strategy shows promise for AKI-D
The LIBERATE-D trial found that this approach led to better renal recovery at discharge vs thrice-weekly dialysis (64% vs 50%)
Although adjusted CIs were nonsignificant and deaths were numerically higher
The LIBERATE-D trial found that this approach led to better renal recovery at discharge vs thrice-weekly dialysis (64% vs 50%)
Although adjusted CIs were nonsignificant and deaths were numerically higher
Reposted by Anil Makam
ICIs for NSCLC illustrates caution in broadening trial eligibility
In ECOG 0-1, trials show overall survival gain (65% vs 50% alive at 18 mos w/ chemo)
In ECOG 2+, excluded in trials & typical of hospitalized adults, survival is just ~4 mos
x.com/EvidenceRounds...
In ECOG 0-1, trials show overall survival gain (65% vs 50% alive at 18 mos w/ chemo)
In ECOG 2+, excluded in trials & typical of hospitalized adults, survival is just ~4 mos
x.com/EvidenceRounds...
November 9, 2025 at 4:25 PM
ICIs for NSCLC illustrates caution in broadening trial eligibility
In ECOG 0-1, trials show overall survival gain (65% vs 50% alive at 18 mos w/ chemo)
In ECOG 2+, excluded in trials & typical of hospitalized adults, survival is just ~4 mos
x.com/EvidenceRounds...
In ECOG 0-1, trials show overall survival gain (65% vs 50% alive at 18 mos w/ chemo)
In ECOG 2+, excluded in trials & typical of hospitalized adults, survival is just ~4 mos
x.com/EvidenceRounds...
Reposted by Anil Makam
Many FDA-approved drugs receive indications broader than pivotal clinical trials, most notably for patient fitness
While broader labels can extend access, absolute benefits may be smaller or absent altogether, especially for sicker & more impaired hospitalized patients
While broader labels can extend access, absolute benefits may be smaller or absent altogether, especially for sicker & more impaired hospitalized patients
November 8, 2025 at 5:54 PM
Many FDA-approved drugs receive indications broader than pivotal clinical trials, most notably for patient fitness
While broader labels can extend access, absolute benefits may be smaller or absent altogether, especially for sicker & more impaired hospitalized patients
While broader labels can extend access, absolute benefits may be smaller or absent altogether, especially for sicker & more impaired hospitalized patients
Reposted by Anil Makam
The rise in early-onset cancer in the US, including colon cancer, is less an epidemic of disease & more an epidemic of diagnosis
The lack of a substantial rise in deaths, despite significant rising incidence strongly suggests increased diagnostic scrutiny & overdiagnosis
The lack of a substantial rise in deaths, despite significant rising incidence strongly suggests increased diagnostic scrutiny & overdiagnosis
November 5, 2025 at 3:35 PM
The rise in early-onset cancer in the US, including colon cancer, is less an epidemic of disease & more an epidemic of diagnosis
The lack of a substantial rise in deaths, despite significant rising incidence strongly suggests increased diagnostic scrutiny & overdiagnosis
The lack of a substantial rise in deaths, despite significant rising incidence strongly suggests increased diagnostic scrutiny & overdiagnosis
Reposted by Anil Makam
Routine use of gabapentin for postoperative pain is not supported by evidence
In a large multicenter double-blind RCT of patients undergoing major surgery, gabapentin did NOT improve pain, opioid use, length of stay, or quality of life
confirms a prior meta-analysis
In a large multicenter double-blind RCT of patients undergoing major surgery, gabapentin did NOT improve pain, opioid use, length of stay, or quality of life
confirms a prior meta-analysis
October 30, 2025 at 3:01 PM
Routine use of gabapentin for postoperative pain is not supported by evidence
In a large multicenter double-blind RCT of patients undergoing major surgery, gabapentin did NOT improve pain, opioid use, length of stay, or quality of life
confirms a prior meta-analysis
In a large multicenter double-blind RCT of patients undergoing major surgery, gabapentin did NOT improve pain, opioid use, length of stay, or quality of life
confirms a prior meta-analysis
Reposted by Anil Makam
Following the topline SNAP trial results, a new multicenter trial found cefazolin noninferior to cloxacillin for MSSA bacteremia, with fewer adverse events
Given its safety, convenience, and lower cost, cefazolin should be considered first-line therapy for MSSA bacteremia
Given its safety, convenience, and lower cost, cefazolin should be considered first-line therapy for MSSA bacteremia
October 28, 2025 at 5:04 PM
Following the topline SNAP trial results, a new multicenter trial found cefazolin noninferior to cloxacillin for MSSA bacteremia, with fewer adverse events
Given its safety, convenience, and lower cost, cefazolin should be considered first-line therapy for MSSA bacteremia
Given its safety, convenience, and lower cost, cefazolin should be considered first-line therapy for MSSA bacteremia
You're gonna wanna follow this
Will be the single best way to have your finger on the pulse of what matters in hospital medicine and inpatient medicine more broadly
Will be the single best way to have your finger on the pulse of what matters in hospital medicine and inpatient medicine more broadly
Welcome to Evidence Rounds!
You might be an Evidence Rounder if you drown in literature that rarely helps and want trustworthy, curated evidence
Follow for weekly updates featuring practice-changing studies and the most promising ideas that shape hospital medicine
You might be an Evidence Rounder if you drown in literature that rarely helps and want trustworthy, curated evidence
Follow for weekly updates featuring practice-changing studies and the most promising ideas that shape hospital medicine
October 28, 2025 at 5:17 PM
You're gonna wanna follow this
Will be the single best way to have your finger on the pulse of what matters in hospital medicine and inpatient medicine more broadly
Will be the single best way to have your finger on the pulse of what matters in hospital medicine and inpatient medicine more broadly
Reposted by Anil Makam

This study seems riddled with selection and detection biases and I can't see how any knowledgeable expert could just take the results at face value and conclude a doubling of risk of long-covid with reinfection.
Children and teens who had a Covid reinfection had a doubling of #LongCovid risk (PASC) and a significant increase in many other adverse outcomes (Figure) www.thelancet.com/journals/lan...

October 2, 2025 at 4:56 AM
This study seems riddled with selection and detection biases and I can't see how any knowledgeable expert could just take the results at face value and conclude a doubling of risk of long-covid with reinfection.
We had our first OFF site Division retreat last week!
Incredible energy, connection & culture building
Plus iconic SF views & food :)
UCSF DHM based at ZSFG is becoming the best academic Division of Hospital Medicine in the country
And not just for a safety-net
We're hiring btw
Incredible energy, connection & culture building
Plus iconic SF views & food :)
UCSF DHM based at ZSFG is becoming the best academic Division of Hospital Medicine in the country
And not just for a safety-net
We're hiring btw




October 2, 2025 at 3:48 AM
We had our first OFF site Division retreat last week!
Incredible energy, connection & culture building
Plus iconic SF views & food :)
UCSF DHM based at ZSFG is becoming the best academic Division of Hospital Medicine in the country
And not just for a safety-net
We're hiring btw
Incredible energy, connection & culture building
Plus iconic SF views & food :)
UCSF DHM based at ZSFG is becoming the best academic Division of Hospital Medicine in the country
And not just for a safety-net
We're hiring btw
Reposted by Anil Makam

Recent FDA actions on Covid vaccines:
1. Novavax approved (👏)
2. Narrowed indications for all (pros and cons)
3. Called for clinical trials (👍)
No doubt we're relying too much on old data to inform clinical practice. Some thoughts on what we gain… and what we risk. blogs.jwatch.org/hiv-id-obser...
1. Novavax approved (👏)
2. Narrowed indications for all (pros and cons)
3. Called for clinical trials (👍)
No doubt we're relying too much on old data to inform clinical practice. Some thoughts on what we gain… and what we risk. blogs.jwatch.org/hiv-id-obser...
The Pros and Cons of the Latest FDA Actions on COVID Vaccines
In case you missed it, last week the FDA granted full approval for the Novavax COVID-19 vaccine. This vaccine, which uses a more traditional protein-plus-adjuvant strategy instead of the mRNA approach...
blogs.jwatch.org
May 24, 2025 at 11:30 AM
Recent FDA actions on Covid vaccines:
1. Novavax approved (👏)
2. Narrowed indications for all (pros and cons)
3. Called for clinical trials (👍)
No doubt we're relying too much on old data to inform clinical practice. Some thoughts on what we gain… and what we risk. blogs.jwatch.org/hiv-id-obser...
1. Novavax approved (👏)
2. Narrowed indications for all (pros and cons)
3. Called for clinical trials (👍)
No doubt we're relying too much on old data to inform clinical practice. Some thoughts on what we gain… and what we risk. blogs.jwatch.org/hiv-id-obser...
Reposted by Anil Makam

Medicaid Patients with Type 2 Diabetes Face Hurdles Getting Cardioprotective Meds

Medicaid Patients with Type 2 Diabetes Face Hurdles Getting Cardioprotective Meds
Medicaid Patients with Type 2 Diabetes Face Hurdles Getting Cardioprotective Meds
[email protected]
Fri, 04/25/2025 - 16:56
Michael O'Riordan
SGLT2 inhibitors and GLP-1 agonists are class 1 medications, but many Medicaid patients have challenges with access.
www.tctmd.com
April 25, 2025 at 9:03 PM
Medicaid Patients with Type 2 Diabetes Face Hurdles Getting Cardioprotective Meds
Reposted by Anil Makam
🚨New Study in Annals🚨
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
Availability of Cardioprotective Medications for Type 2 Diabetes in the Medicaid Program | Annals of Internal Medicine
Background: Sodium–glucose cotransporter-2 inhibitors (SGLT2is) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are the only type 2 diabetes medications that reduce cardiovascular disease an...
www.acpjournals.org
April 23, 2025 at 8:38 PM
🚨New Study in Annals🚨
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
🚨New Study in Annals🚨
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
Availability of Cardioprotective Medications for Type 2 Diabetes in the Medicaid Program | Annals of Internal Medicine
Background: Sodium–glucose cotransporter-2 inhibitors (SGLT2is) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are the only type 2 diabetes medications that reduce cardiovascular disease an...
www.acpjournals.org
April 23, 2025 at 8:38 PM
🚨New Study in Annals🚨
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
GLP1ra & SGLT2i are the only diabetes meds that reduce heart attacks & death
But can't work if can't prescribe
TLDR
40% Medicaid enrollees have restricted access to GLP1 & 25% to SGLT2i
much state/plan variability
GLP access plateaued in '22
bit.ly/3Y72K2z
Reposted by Anil Makam

Shared without comment.
March 19, 2025 at 11:18 PM
Shared without comment.
I've been thinking more and more about evidence-based diagnosis
Penned this piece with Gurpreet & Oanh on the SSRN preprint server titled:
Striving for Diagnostic Excellence: "The Median Is Not the Message"
Tell me what you think
Penned this piece with Gurpreet & Oanh on the SSRN preprint server titled:
Striving for Diagnostic Excellence: "The Median Is Not the Message"
Tell me what you think
February 5, 2025 at 9:09 PM
I've been thinking more and more about evidence-based diagnosis
Penned this piece with Gurpreet & Oanh on the SSRN preprint server titled:
Striving for Diagnostic Excellence: "The Median Is Not the Message"
Tell me what you think
Penned this piece with Gurpreet & Oanh on the SSRN preprint server titled:
Striving for Diagnostic Excellence: "The Median Is Not the Message"
Tell me what you think
Agree. Not enjoyable so far. Place is great if you like echo chambers, especially ones that celebrate an assassination because of the industry. Thought the selling point was more sanity and compassion? Will lurk time to time to see if gets better, but find me at the other place

The Discover feed is pretty terrible, and I am not sure how to guide the algorithm to make it better.
I know I can use various lists, but I really want a feed that includes serendipity, trends, and a broader set of topics than the one that I follow but isn't full of noise. How do you get that?
I know I can use various lists, but I really want a feed that includes serendipity, trends, and a broader set of topics than the one that I follow but isn't full of noise. How do you get that?
December 5, 2024 at 6:18 AM
Agree. Not enjoyable so far. Place is great if you like echo chambers, especially ones that celebrate an assassination because of the industry. Thought the selling point was more sanity and compassion? Will lurk time to time to see if gets better, but find me at the other place
Here. But really there
November 19, 2024 at 11:42 PM
Here. But really there