




Mark Meiselbach
@markmeiselbach.bsky.social
Assistant Professor studying health economics at Johns Hopkins Bloomberg School of Public Health, Department of Health Policy and Management
I am looking forward to future work on this project to explore enrollee retention and satisfaction in the plans and heterogeneous enrollment effects.
We are grateful for funding from @arnoldventures.bsky.social that supports this work!
We are grateful for funding from @arnoldventures.bsky.social that supports this work!
June 6, 2025 at 7:52 PM
I am looking forward to future work on this project to explore enrollee retention and satisfaction in the plans and heterogeneous enrollment effects.
We are grateful for funding from @arnoldventures.bsky.social that supports this work!
We are grateful for funding from @arnoldventures.bsky.social that supports this work!
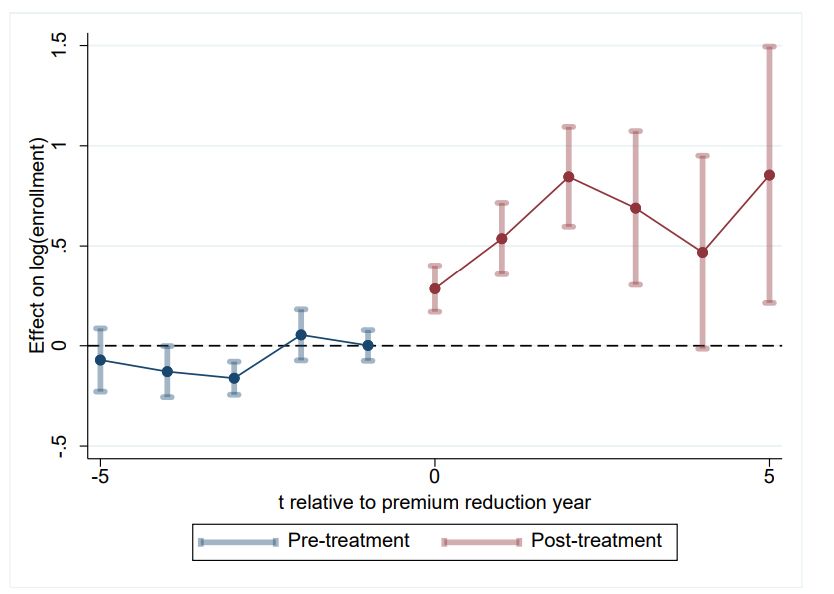
We estimate that hundreds of millions are attributable to this benefit per month in 2024. Further, we find that the introduction of the giveback has a substantial effect on plan enrollment, with enrollment increasing >30% following the offer.
June 6, 2025 at 7:52 PM
We estimate that hundreds of millions are attributable to this benefit per month in 2024. Further, we find that the introduction of the giveback has a substantial effect on plan enrollment, with enrollment increasing >30% following the offer.
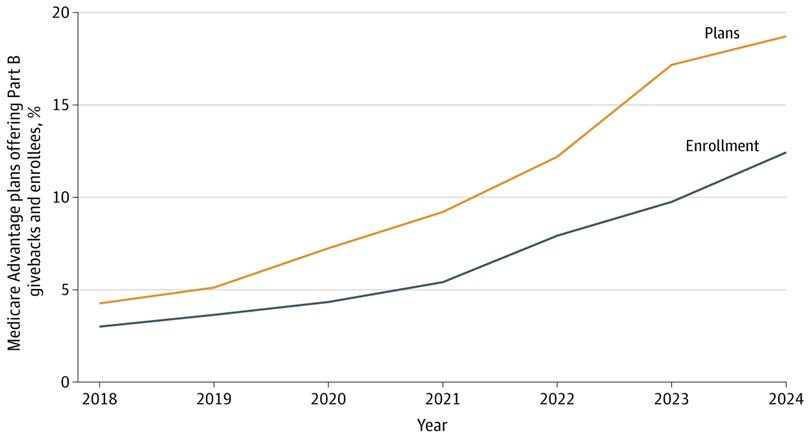
In MA, enrollees still pay Part B premiums even when a plan is "free." This can be $100s per month. Increasingly, plans have been using rebate dollars to "give back" Part B premiums to enrollees in their plans. This is becoming common, with ~19% of plans offering this benefit.
June 6, 2025 at 7:52 PM
In MA, enrollees still pay Part B premiums even when a plan is "free." This can be $100s per month. Increasingly, plans have been using rebate dollars to "give back" Part B premiums to enrollees in their plans. This is becoming common, with ~19% of plans offering this benefit.
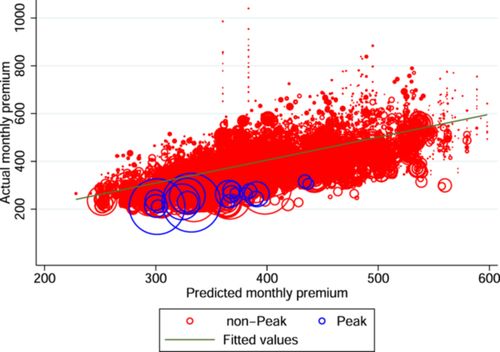
Our findings also suggest that premium reductions were likely driven by price reductions, as opposed to differences in plan design.
There are a number of aspects that made this coalition unique. However, our findings point to the potential effectiveness of the approach.
There are a number of aspects that made this coalition unique. However, our findings point to the potential effectiveness of the approach.
March 3, 2025 at 4:11 PM
Our findings also suggest that premium reductions were likely driven by price reductions, as opposed to differences in plan design.
There are a number of aspects that made this coalition unique. However, our findings point to the potential effectiveness of the approach.
There are a number of aspects that made this coalition unique. However, our findings point to the potential effectiveness of the approach.
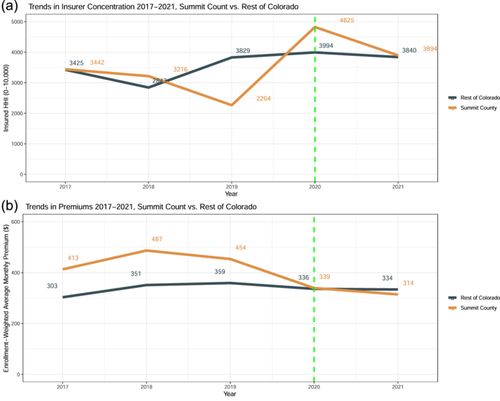
We evaluate the Peak Health Alliance in Colorado, which began offering plans in 2020. With 2017–2021 plan data provided by the CO DORA, we found that Peak's rollout led to a 13%–17% decrease in average premiums in 2020-2021.
March 3, 2025 at 4:11 PM
We evaluate the Peak Health Alliance in Colorado, which began offering plans in 2020. With 2017–2021 plan data provided by the CO DORA, we found that Peak's rollout led to a 13%–17% decrease in average premiums in 2020-2021.
Our next steps will be to understand the drivers of these trends and understand the costs to expenditures at the state, federal, and individual level.
We are very grateful to @arnoldventures.bsky.social for funding this work.
We are very grateful to @arnoldventures.bsky.social for funding this work.
January 17, 2025 at 9:50 PM
Our next steps will be to understand the drivers of these trends and understand the costs to expenditures at the state, federal, and individual level.
We are very grateful to @arnoldventures.bsky.social for funding this work.
We are very grateful to @arnoldventures.bsky.social for funding this work.
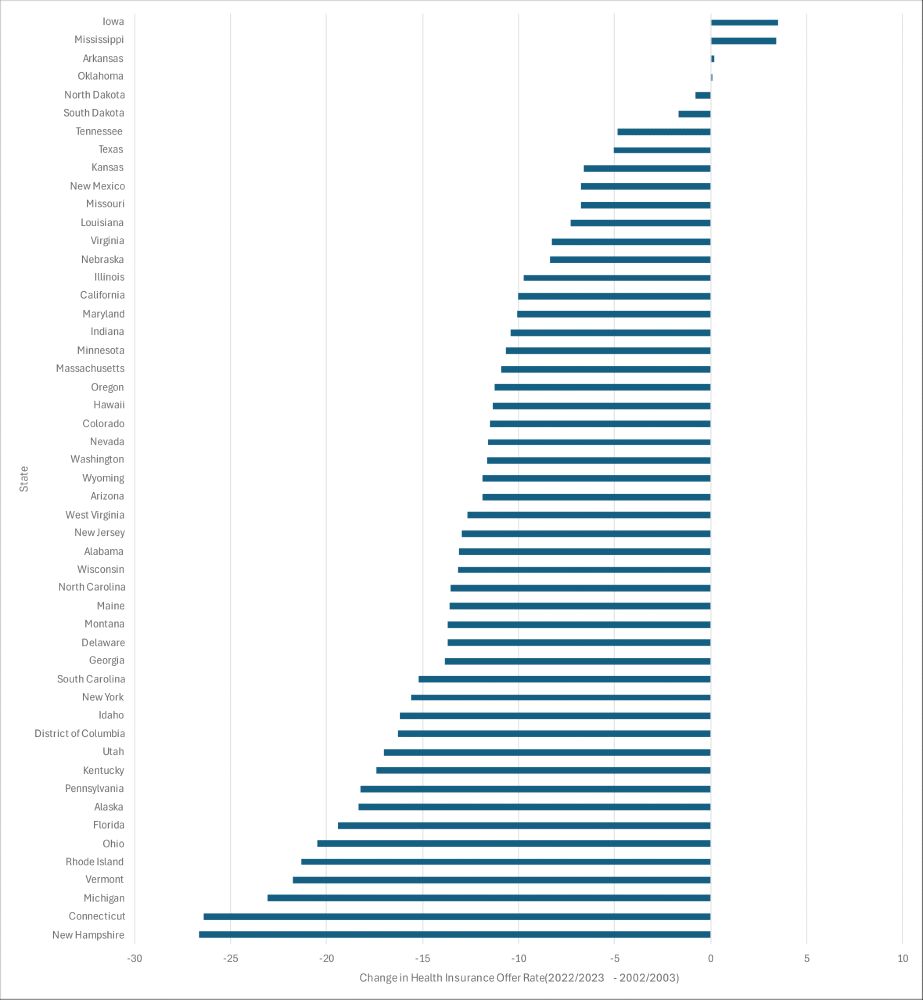
We discuss the variation in this trend across states (see below). While there are some known causes, the drivers of this state-to-state variation is largely unknown. Further, how important is this? What are the costs? This is all vital to study, yet often unexamined.
January 17, 2025 at 9:50 PM
We discuss the variation in this trend across states (see below). While there are some known causes, the drivers of this state-to-state variation is largely unknown. Further, how important is this? What are the costs? This is all vital to study, yet often unexamined.
We did our best to identify all the "affinity plans" that we could, not including plans for VA and Medicaid beneficiaries which are somewhat different. Our list is public and we hope that other can use the list, build off of it, and refine: archive.data.jhu.edu/dataset.xhtm...
archive.data.jhu.edu
December 3, 2024 at 5:02 PM
We did our best to identify all the "affinity plans" that we could, not including plans for VA and Medicaid beneficiaries which are somewhat different. Our list is public and we hope that other can use the list, build off of it, and refine: archive.data.jhu.edu/dataset.xhtm...
Finding #2: based on MA star rating system, the plans are generally of lower average quality or unrated. But not too surprising. The plans are very new, with >60% linked to a contract starting in 2021 or later.
December 3, 2024 at 5:02 PM
Finding #2: based on MA star rating system, the plans are generally of lower average quality or unrated. But not too surprising. The plans are very new, with >60% linked to a contract starting in 2021 or later.
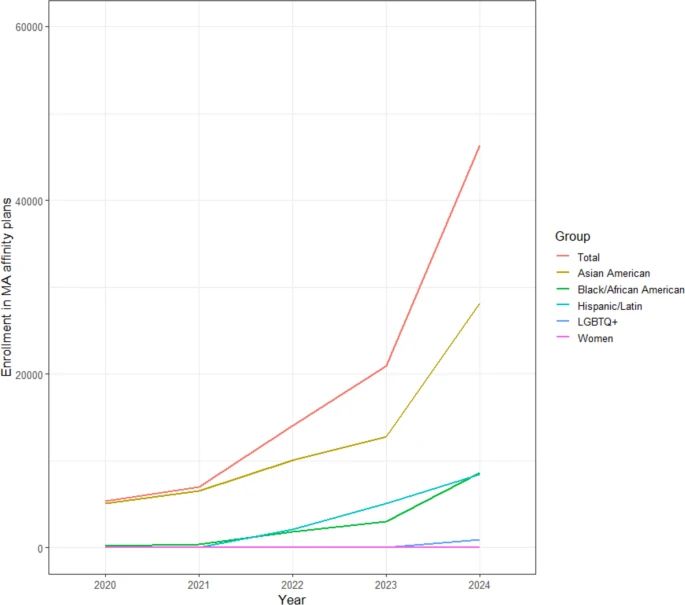
Finding #1: these plans still have a small footprint (~50k enrollees), but it's rapidly growing. Enrollment is more than doubling year over year. The largest category are plans designed specifically for Asian American beneficiaries.
December 3, 2024 at 5:02 PM
Finding #1: these plans still have a small footprint (~50k enrollees), but it's rapidly growing. Enrollment is more than doubling year over year. The largest category are plans designed specifically for Asian American beneficiaries.
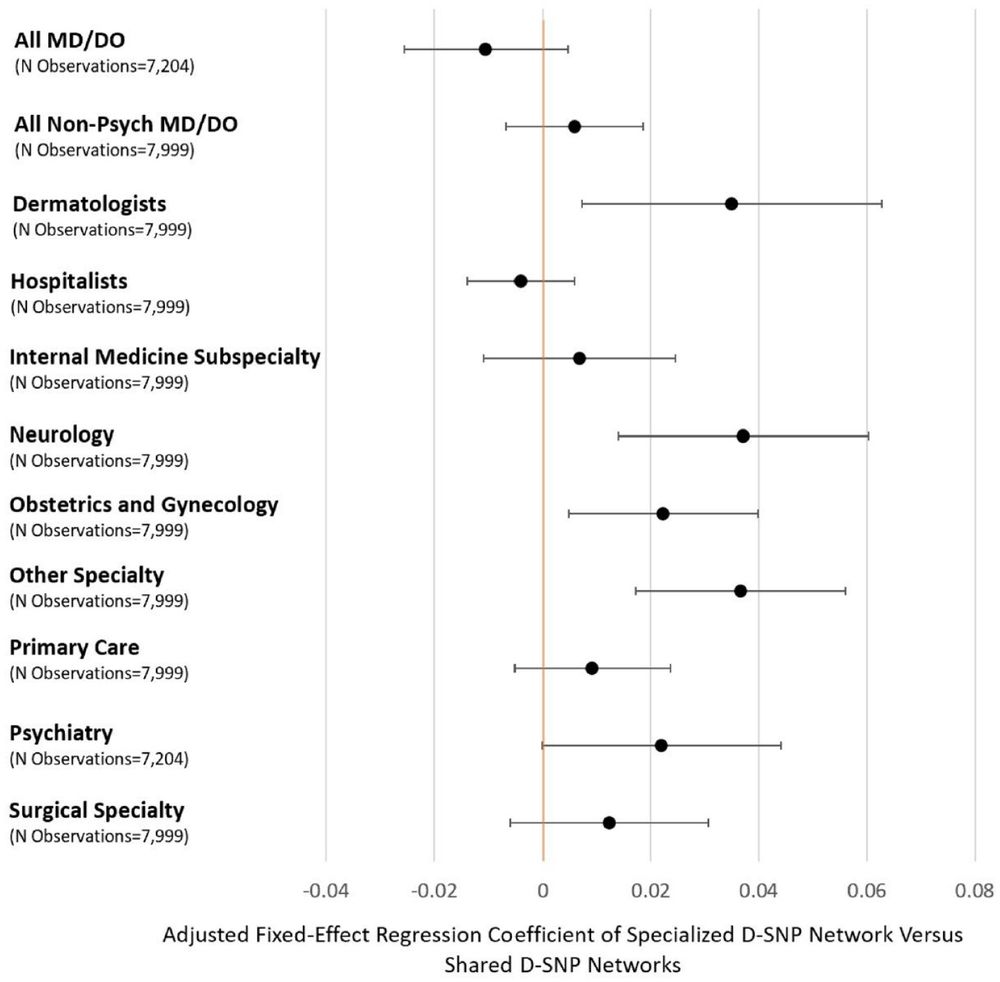
3. When D-SNP networks were specialized, they tended to include a larger share of specialists that commonly treat conditions more prevalent among dually eligible enrollees.
November 20, 2024 at 6:35 PM
3. When D-SNP networks were specialized, they tended to include a larger share of specialists that commonly treat conditions more prevalent among dually eligible enrollees.
I learned a lot from this paper. Some key findings.
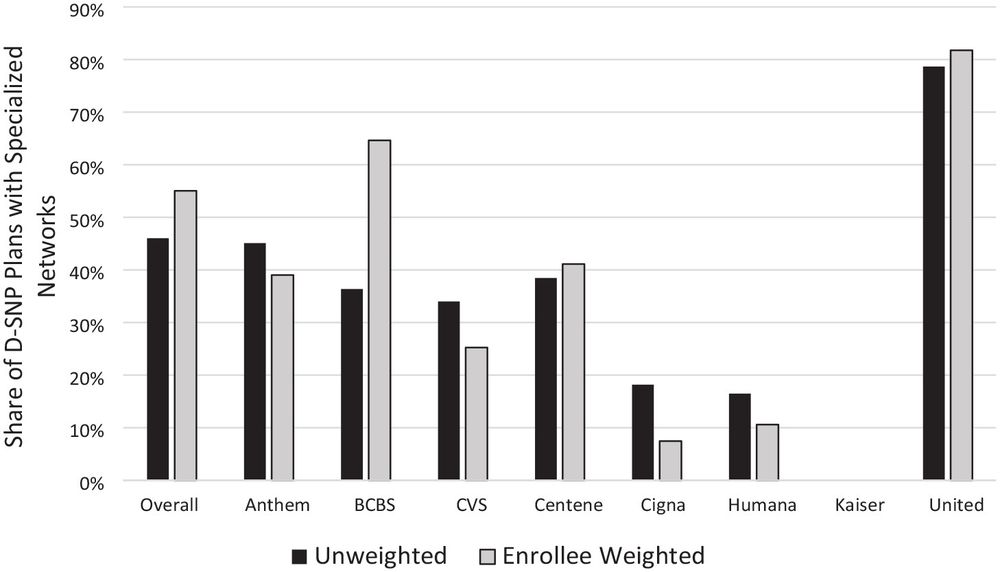
1. Only about half D-SNP plan provider networks were at all distinct from provider networks in standard MA plans offered by the same insurer.
2. These specialized networks were much more common among Fully Integrated Dual Eligible Plans (FIDEs).
1. Only about half D-SNP plan provider networks were at all distinct from provider networks in standard MA plans offered by the same insurer.
2. These specialized networks were much more common among Fully Integrated Dual Eligible Plans (FIDEs).
November 20, 2024 at 6:35 PM
I learned a lot from this paper. Some key findings.
1. Only about half D-SNP plan provider networks were at all distinct from provider networks in standard MA plans offered by the same insurer.
2. These specialized networks were much more common among Fully Integrated Dual Eligible Plans (FIDEs).
1. Only about half D-SNP plan provider networks were at all distinct from provider networks in standard MA plans offered by the same insurer.
2. These specialized networks were much more common among Fully Integrated Dual Eligible Plans (FIDEs).
Oops - need to check this app more often. I don’t know of publicly available aggregate data but they can be derived from claims. For example, the nicely named below paper used IQVIA. You can see the back and forth between providers/insurers: academic.oup.com/qje
March 24, 2024 at 8:12 PM
Oops - need to check this app more often. I don’t know of publicly available aggregate data but they can be derived from claims. For example, the nicely named below paper used IQVIA. You can see the back and forth between providers/insurers: academic.oup.com/qje