



@kaulcsmc.bsky.social
Cardiologist, evidence appraiser, data detective, rock music fan
Shmeta-analysis.
June 5, 2025 at 6:06 PM
Shmeta-analysis.
Post-treatment discontinuation eGFR trajectory is somewhat reassuring. No?
June 5, 2025 at 4:08 PM
Post-treatment discontinuation eGFR trajectory is somewhat reassuring. No?
I think it is a positive first step, but whether there is a convincing evidence of an additive effect of combination therapy requires proof in an outcome study.
For now, combination therapy has won the bragging rights, but I would not go so far as to proclaim this is a practice-changing trial.
For now, combination therapy has won the bragging rights, but I would not go so far as to proclaim this is a practice-changing trial.
June 5, 2025 at 3:47 PM
I think it is a positive first step, but whether there is a convincing evidence of an additive effect of combination therapy requires proof in an outcome study.
For now, combination therapy has won the bragging rights, but I would not go so far as to proclaim this is a practice-changing trial.
For now, combination therapy has won the bragging rights, but I would not go so far as to proclaim this is a practice-changing trial.
Is there a dose-response or a threshold relationship with UACR reduction and clinical outcome benefit? In other words, will a >50% reduction translate into a greater kidney or CV benefit than >30% reduction?
June 5, 2025 at 2:59 PM
Is there a dose-response or a threshold relationship with UACR reduction and clinical outcome benefit? In other words, will a >50% reduction translate into a greater kidney or CV benefit than >30% reduction?
Hyperkalemia on combo vs nsMRA: RR 0.82, 95% CI 0.50-1.36
No clearcut evidence that hyperkalemia risk is mitigated by combining sglt2i with nsMRA (? Inadequate power/Sample Size)
No clearcut evidence that hyperkalemia risk is mitigated by combining sglt2i with nsMRA (? Inadequate power/Sample Size)
June 5, 2025 at 2:31 PM
Hyperkalemia on combo vs nsMRA: RR 0.82, 95% CI 0.50-1.36
No clearcut evidence that hyperkalemia risk is mitigated by combining sglt2i with nsMRA (? Inadequate power/Sample Size)
No clearcut evidence that hyperkalemia risk is mitigated by combining sglt2i with nsMRA (? Inadequate power/Sample Size)
Pragmatic trials like comparative effectiveness studies require realistically ‘sober’ assumptions to account for the issues you stated.
Lipid hypothesis lingered on for several decades until LDL-C lowering was proven to reduce CV risk. Analogy applies to INOCA/ANOCA/MINOCA. Need novel targeted Rxs.
Lipid hypothesis lingered on for several decades until LDL-C lowering was proven to reduce CV risk. Analogy applies to INOCA/ANOCA/MINOCA. Need novel targeted Rxs.
March 30, 2025 at 11:20 PM
Pragmatic trials like comparative effectiveness studies require realistically ‘sober’ assumptions to account for the issues you stated.
Lipid hypothesis lingered on for several decades until LDL-C lowering was proven to reduce CV risk. Analogy applies to INOCA/ANOCA/MINOCA. Need novel targeted Rxs.
Lipid hypothesis lingered on for several decades until LDL-C lowering was proven to reduce CV risk. Analogy applies to INOCA/ANOCA/MINOCA. Need novel targeted Rxs.
95% CI is compatible with a 6% benefit (clinically trivial) to 37% harm (clinically important). If CI contained a clinically important benefit, say HR of 0.80 or a more plausible HR of 0.85 to 0.90, but CI was wide spanning across HR of 1, then an inference of inconclusive result would be justified.
March 30, 2025 at 11:16 PM
95% CI is compatible with a 6% benefit (clinically trivial) to 37% harm (clinically important). If CI contained a clinically important benefit, say HR of 0.80 or a more plausible HR of 0.85 to 0.90, but CI was wide spanning across HR of 1, then an inference of inconclusive result would be justified.
Trial powered for a HR of 0.80 which was excluded by the 95% CI.
Is it still a null outcome?
Is it still a null outcome?
March 29, 2025 at 3:03 PM
Trial powered for a HR of 0.80 which was excluded by the 95% CI.
Is it still a null outcome?
Is it still a null outcome?
Who are the optimal candidates for acoramidis therapy?
When should it be considered first-line therapy?
Does the proposed cost provide value?
When should it be considered first-line therapy?
Does the proposed cost provide value?
November 23, 2024 at 1:42 AM
Who are the optimal candidates for acoramidis therapy?
When should it be considered first-line therapy?
Does the proposed cost provide value?
When should it be considered first-line therapy?
Does the proposed cost provide value?
NI margin in EVEREST II trial of MitraClip vs MV surgery for MR was 31% absolute difference, a margin through which one could drive 3 buses lined side by side.
Trial met NI despite the fact that HR excluded 1.0, i.e., MitraClip was INFERIOR to surgery, yet NONINFERIOR!
www.nejm.org/doi/full/10....
Trial met NI despite the fact that HR excluded 1.0, i.e., MitraClip was INFERIOR to surgery, yet NONINFERIOR!
www.nejm.org/doi/full/10....
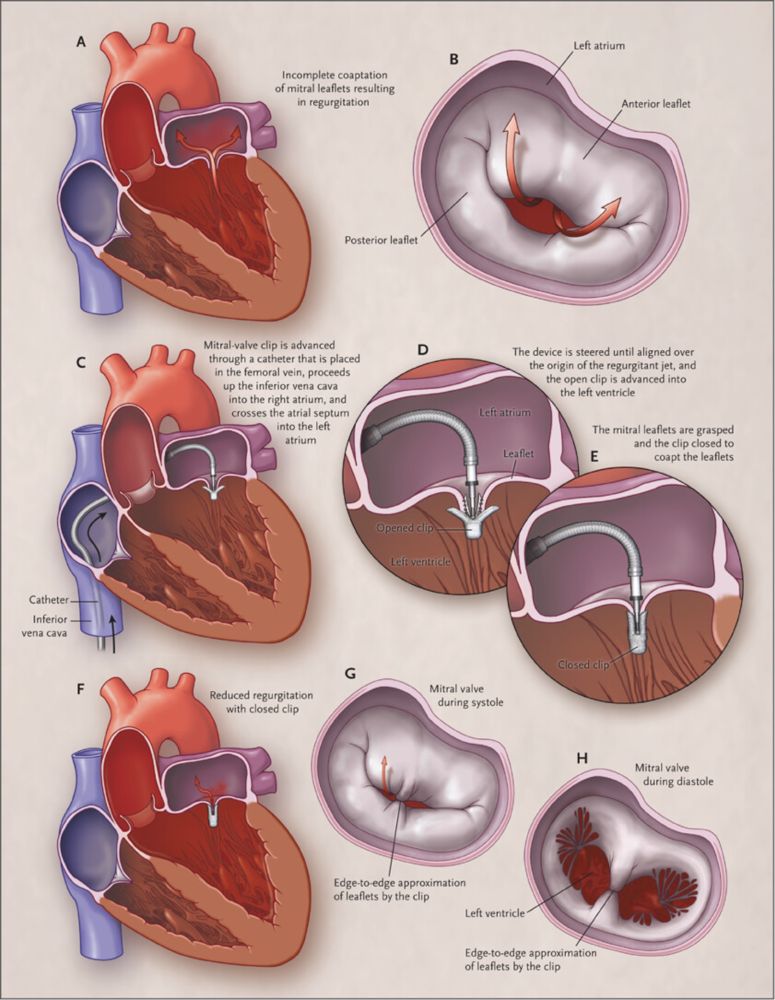
Percutaneous Repair or Surgery for Mitral Regurgitation | NEJM
Mitral-valve repair can be accomplished with an investigational procedure that involves the percutaneous implantation of a clip that grasps and approximates the edges of the mitral leaflets at the ...
www.nejm.org
November 22, 2024 at 2:33 AM
NI margin in EVEREST II trial of MitraClip vs MV surgery for MR was 31% absolute difference, a margin through which one could drive 3 buses lined side by side.
Trial met NI despite the fact that HR excluded 1.0, i.e., MitraClip was INFERIOR to surgery, yet NONINFERIOR!
www.nejm.org/doi/full/10....
Trial met NI despite the fact that HR excluded 1.0, i.e., MitraClip was INFERIOR to surgery, yet NONINFERIOR!
www.nejm.org/doi/full/10....
Even though the observed rates were lower than assumed (22%), had NI margin been fixed as risk ratio of 1.18 ([22+4]/22), the overall results would still have met NI as RR was 0.90, 0.77-1.05. An excellent example of how a NI trial should be designed and executed. Congrats to trial investigators.
November 22, 2024 at 2:17 AM
Even though the observed rates were lower than assumed (22%), had NI margin been fixed as risk ratio of 1.18 ([22+4]/22), the overall results would still have met NI as RR was 0.90, 0.77-1.05. An excellent example of how a NI trial should be designed and executed. Congrats to trial investigators.
So you are suggesting you need longer f/u and greater LDL and Lp(a) reduction, both of which favor PREVAIL. So what is the probability of success?
November 20, 2024 at 9:23 PM
So you are suggesting you need longer f/u and greater LDL and Lp(a) reduction, both of which favor PREVAIL. So what is the probability of success?
4/
Key Qs
What is probability of success with obicetrapib?
Why should obicetrapib succeed when 2 other CETPi did not?
Is absolute or relative LDL reduction key driver of benefit?
Is duration of treatment important?
Is LDL lowering with CETPi different from other LDL lowering Rx?
Key Qs
What is probability of success with obicetrapib?
Why should obicetrapib succeed when 2 other CETPi did not?
Is absolute or relative LDL reduction key driver of benefit?
Is duration of treatment important?
Is LDL lowering with CETPi different from other LDL lowering Rx?
November 20, 2024 at 5:42 AM
4/
Key Qs
What is probability of success with obicetrapib?
Why should obicetrapib succeed when 2 other CETPi did not?
Is absolute or relative LDL reduction key driver of benefit?
Is duration of treatment important?
Is LDL lowering with CETPi different from other LDL lowering Rx?
Key Qs
What is probability of success with obicetrapib?
Why should obicetrapib succeed when 2 other CETPi did not?
Is absolute or relative LDL reduction key driver of benefit?
Is duration of treatment important?
Is LDL lowering with CETPi different from other LDL lowering Rx?
3/
PREVAIL(Obicetrapib), N=9541, F/U: ~4y
Mean LDL 103; LDL⬇️35-40%, Lp(a)⬇️45% (based on BROOKLYN)
PEP (4-MACE): Powered for 15-20% RRR
Recruitment completed; event-driven trial
Targeting higher baseline LDL & higher risk patients
PREVAIL(Obicetrapib), N=9541, F/U: ~4y
Mean LDL 103; LDL⬇️35-40%, Lp(a)⬇️45% (based on BROOKLYN)
PEP (4-MACE): Powered for 15-20% RRR
Recruitment completed; event-driven trial
Targeting higher baseline LDL & higher risk patients
November 20, 2024 at 5:42 AM
3/
PREVAIL(Obicetrapib), N=9541, F/U: ~4y
Mean LDL 103; LDL⬇️35-40%, Lp(a)⬇️45% (based on BROOKLYN)
PEP (4-MACE): Powered for 15-20% RRR
Recruitment completed; event-driven trial
Targeting higher baseline LDL & higher risk patients
PREVAIL(Obicetrapib), N=9541, F/U: ~4y
Mean LDL 103; LDL⬇️35-40%, Lp(a)⬇️45% (based on BROOKLYN)
PEP (4-MACE): Powered for 15-20% RRR
Recruitment completed; event-driven trial
Targeting higher baseline LDL & higher risk patients
2/
REVEAL (Anacetrapib), N=30,449, F/U: 4.1y
Mean LDL 61; LDL⬇️41%, Lp(a)⬇️25%
PEP (3-MACE): 10.8% vs 11.8%, HR 0.91, 0.85-0.97
Development halted (long half-life, modest Rx effect)
REVEAL (Anacetrapib), N=30,449, F/U: 4.1y
Mean LDL 61; LDL⬇️41%, Lp(a)⬇️25%
PEP (3-MACE): 10.8% vs 11.8%, HR 0.91, 0.85-0.97
Development halted (long half-life, modest Rx effect)
November 20, 2024 at 5:42 AM
2/
REVEAL (Anacetrapib), N=30,449, F/U: 4.1y
Mean LDL 61; LDL⬇️41%, Lp(a)⬇️25%
PEP (3-MACE): 10.8% vs 11.8%, HR 0.91, 0.85-0.97
Development halted (long half-life, modest Rx effect)
REVEAL (Anacetrapib), N=30,449, F/U: 4.1y
Mean LDL 61; LDL⬇️41%, Lp(a)⬇️25%
PEP (3-MACE): 10.8% vs 11.8%, HR 0.91, 0.85-0.97
Development halted (long half-life, modest Rx effect)