



Amy Pomeroy
@amypomeroy.bsky.social
computational cancer pharmacologist at UNC | modeling clinical trials of combination therapy
13/13
There are so many people to thank for their contributions to this work. Most importantly my advisor Adam Palmer. I'd also like to thank @unclineberger.bsky.social and @unc-phco.bsky.social (and a lot of other individuals and organizations not on bluesky).
There are so many people to thank for their contributions to this work. Most importantly my advisor Adam Palmer. I'd also like to thank @unclineberger.bsky.social and @unc-phco.bsky.social (and a lot of other individuals and organizations not on bluesky).
April 10, 2025 at 3:57 PM
13/13
There are so many people to thank for their contributions to this work. Most importantly my advisor Adam Palmer. I'd also like to thank @unclineberger.bsky.social and @unc-phco.bsky.social (and a lot of other individuals and organizations not on bluesky).
There are so many people to thank for their contributions to this work. Most importantly my advisor Adam Palmer. I'd also like to thank @unclineberger.bsky.social and @unc-phco.bsky.social (and a lot of other individuals and organizations not on bluesky).
12/n
This model provides quantitative insight into how combination therapy can overcome heterogeneity within and between tumors to cure many patients with Large B-Cell Lymphoma.
We hope it is a practical tool to explore new combinations based on clinical data on new drugs.
This model provides quantitative insight into how combination therapy can overcome heterogeneity within and between tumors to cure many patients with Large B-Cell Lymphoma.
We hope it is a practical tool to explore new combinations based on clinical data on new drugs.
April 10, 2025 at 3:57 PM
12/n
This model provides quantitative insight into how combination therapy can overcome heterogeneity within and between tumors to cure many patients with Large B-Cell Lymphoma.
We hope it is a practical tool to explore new combinations based on clinical data on new drugs.
This model provides quantitative insight into how combination therapy can overcome heterogeneity within and between tumors to cure many patients with Large B-Cell Lymphoma.
We hope it is a practical tool to explore new combinations based on clinical data on new drugs.
11/n
Importantly, we had predicted the success of Pola-R-CHP *before* the trial read out, as she reported from the model prototype back in 2021:
www.amypomeroy.com/post/predict...
Importantly, we had predicted the success of Pola-R-CHP *before* the trial read out, as she reported from the model prototype back in 2021:
www.amypomeroy.com/post/predict...

Predicting the results of the POLARIX trial
Diffuse Large B-Cell Lymphoma (DLBCL) is the most common blood cancer with 18,000 new diagnoses each year (lymphoma.org). It is typically treated with the five-drug combination R-CHOP, which includes ...
www.amypomeroy.com
April 10, 2025 at 3:57 PM
11/n
Importantly, we had predicted the success of Pola-R-CHP *before* the trial read out, as she reported from the model prototype back in 2021:
www.amypomeroy.com/post/predict...
Importantly, we had predicted the success of Pola-R-CHP *before* the trial read out, as she reported from the model prototype back in 2021:
www.amypomeroy.com/post/predict...
10/n
Looking at ‘RCHOP+X’ trials, we used clinical data on each ‘drug X’ to predict the clinical trial results.
Only Pola-R-CHP, and Tucidinostat + R-CHOP, were expected to succeed, and indeed they did
www.asco.org/abstracts-presentations/ABSTRACT451754
www.nejm.org/doi/full/10.1056/NEJMoa2115304
Looking at ‘RCHOP+X’ trials, we used clinical data on each ‘drug X’ to predict the clinical trial results.
Only Pola-R-CHP, and Tucidinostat + R-CHOP, were expected to succeed, and indeed they did
www.asco.org/abstracts-presentations/ABSTRACT451754
www.nejm.org/doi/full/10.1056/NEJMoa2115304

April 10, 2025 at 3:57 PM
10/n
Looking at ‘RCHOP+X’ trials, we used clinical data on each ‘drug X’ to predict the clinical trial results.
Only Pola-R-CHP, and Tucidinostat + R-CHOP, were expected to succeed, and indeed they did
www.asco.org/abstracts-presentations/ABSTRACT451754
www.nejm.org/doi/full/10.1056/NEJMoa2115304
Looking at ‘RCHOP+X’ trials, we used clinical data on each ‘drug X’ to predict the clinical trial results.
Only Pola-R-CHP, and Tucidinostat + R-CHOP, were expected to succeed, and indeed they did
www.asco.org/abstracts-presentations/ABSTRACT451754
www.nejm.org/doi/full/10.1056/NEJMoa2115304
9/n
We calibrated the model to reproduce Progression-Free Survival for the CHOP and RCHOP regimens for Diffuse Large B-Cell Lymphoma.
Simulated tumor population shrinkage agreed well with observed changes in circulating tumor DNA after the first cycle of RCHOP:
We calibrated the model to reproduce Progression-Free Survival for the CHOP and RCHOP regimens for Diffuse Large B-Cell Lymphoma.
Simulated tumor population shrinkage agreed well with observed changes in circulating tumor DNA after the first cycle of RCHOP:

April 10, 2025 at 3:57 PM
9/n
We calibrated the model to reproduce Progression-Free Survival for the CHOP and RCHOP regimens for Diffuse Large B-Cell Lymphoma.
Simulated tumor population shrinkage agreed well with observed changes in circulating tumor DNA after the first cycle of RCHOP:
We calibrated the model to reproduce Progression-Free Survival for the CHOP and RCHOP regimens for Diffuse Large B-Cell Lymphoma.
Simulated tumor population shrinkage agreed well with observed changes in circulating tumor DNA after the first cycle of RCHOP:
8/n
From this ‘bottom-up’ model of tumor heterogeneity, simulating treatment responses in a cohort of patients produces a Kaplan-Meier curve of Progression-Free Survival:
From this ‘bottom-up’ model of tumor heterogeneity, simulating treatment responses in a cohort of patients produces a Kaplan-Meier curve of Progression-Free Survival:

April 10, 2025 at 3:57 PM
8/n
From this ‘bottom-up’ model of tumor heterogeneity, simulating treatment responses in a cohort of patients produces a Kaplan-Meier curve of Progression-Free Survival:
From this ‘bottom-up’ model of tumor heterogeneity, simulating treatment responses in a cohort of patients produces a Kaplan-Meier curve of Progression-Free Survival:
7/n
This extends to combination therapy by using a different dimension of heterogeneity for each drug
This way, patients and cells vary in their sensitivity to different drugs; for example, some patients can be more sensitive to one drug than another, or sensitive to both, etc.
This extends to combination therapy by using a different dimension of heterogeneity for each drug
This way, patients and cells vary in their sensitivity to different drugs; for example, some patients can be more sensitive to one drug than another, or sensitive to both, etc.

April 10, 2025 at 3:57 PM
7/n
This extends to combination therapy by using a different dimension of heterogeneity for each drug
This way, patients and cells vary in their sensitivity to different drugs; for example, some patients can be more sensitive to one drug than another, or sensitive to both, etc.
This extends to combination therapy by using a different dimension of heterogeneity for each drug
This way, patients and cells vary in their sensitivity to different drugs; for example, some patients can be more sensitive to one drug than another, or sensitive to both, etc.
6/n
Extending to patient variability, a group of patients - say in a clinical trial - also have a distribution of drug response phenotypes, with each patient’s cancer containing a range of cellular heterogeneity around the average drug sensitivity of that individual.
Extending to patient variability, a group of patients - say in a clinical trial - also have a distribution of drug response phenotypes, with each patient’s cancer containing a range of cellular heterogeneity around the average drug sensitivity of that individual.

April 10, 2025 at 3:57 PM
6/n
Extending to patient variability, a group of patients - say in a clinical trial - also have a distribution of drug response phenotypes, with each patient’s cancer containing a range of cellular heterogeneity around the average drug sensitivity of that individual.
Extending to patient variability, a group of patients - say in a clinical trial - also have a distribution of drug response phenotypes, with each patient’s cancer containing a range of cellular heterogeneity around the average drug sensitivity of that individual.
5/n
In this model of heterogeneity as a distribution of states, each cycle of chemotherapy progressively shifts the distribution to increasingly drug-resistant states
In this model of heterogeneity as a distribution of states, each cycle of chemotherapy progressively shifts the distribution to increasingly drug-resistant states

April 10, 2025 at 3:57 PM
5/n
In this model of heterogeneity as a distribution of states, each cycle of chemotherapy progressively shifts the distribution to increasingly drug-resistant states
In this model of heterogeneity as a distribution of states, each cycle of chemotherapy progressively shifts the distribution to increasingly drug-resistant states
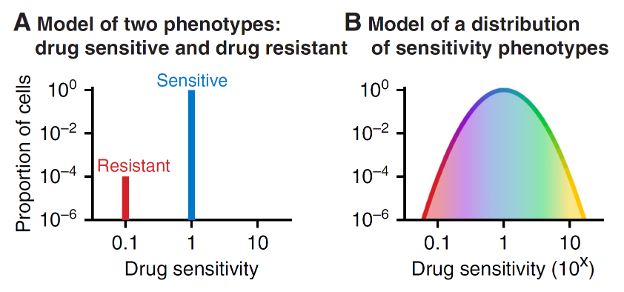
4/n
Many insightful models of tumor heterogeneity described drug-sensitive and drug-resistant subpopulations.
Based on clone-tracing, we modelled cellular heterogeneity as a distribution of sensitivity phenotypes, reflecting many complex influences on drug response
Many insightful models of tumor heterogeneity described drug-sensitive and drug-resistant subpopulations.
Based on clone-tracing, we modelled cellular heterogeneity as a distribution of sensitivity phenotypes, reflecting many complex influences on drug response
April 10, 2025 at 3:57 PM
4/n
Many insightful models of tumor heterogeneity described drug-sensitive and drug-resistant subpopulations.
Based on clone-tracing, we modelled cellular heterogeneity as a distribution of sensitivity phenotypes, reflecting many complex influences on drug response
Many insightful models of tumor heterogeneity described drug-sensitive and drug-resistant subpopulations.
Based on clone-tracing, we modelled cellular heterogeneity as a distribution of sensitivity phenotypes, reflecting many complex influences on drug response
3/n
We built a model that unifies intra-tumor and inter-patient heterogeneity in drug sensitivity to understand the clinical efficacy of curative-intent combination therapy for Large B-Cell Lymphoma.
We built a model that unifies intra-tumor and inter-patient heterogeneity in drug sensitivity to understand the clinical efficacy of curative-intent combination therapy for Large B-Cell Lymphoma.
April 10, 2025 at 3:57 PM
3/n
We built a model that unifies intra-tumor and inter-patient heterogeneity in drug sensitivity to understand the clinical efficacy of curative-intent combination therapy for Large B-Cell Lymphoma.
We built a model that unifies intra-tumor and inter-patient heterogeneity in drug sensitivity to understand the clinical efficacy of curative-intent combination therapy for Large B-Cell Lymphoma.
2/n
Cell-to-cell and patient-to-patient heterogeneity both have a role in the success of drug combinations.
While inter-patient variation can explain better response rates of combos for incurable cancers, CURES need a regimen to overcome cellular heterogeneity and evolution.
Cell-to-cell and patient-to-patient heterogeneity both have a role in the success of drug combinations.
While inter-patient variation can explain better response rates of combos for incurable cancers, CURES need a regimen to overcome cellular heterogeneity and evolution.
April 10, 2025 at 3:57 PM
2/n
Cell-to-cell and patient-to-patient heterogeneity both have a role in the success of drug combinations.
While inter-patient variation can explain better response rates of combos for incurable cancers, CURES need a regimen to overcome cellular heterogeneity and evolution.
Cell-to-cell and patient-to-patient heterogeneity both have a role in the success of drug combinations.
While inter-patient variation can explain better response rates of combos for incurable cancers, CURES need a regimen to overcome cellular heterogeneity and evolution.
Reposted by Amy Pomeroy

An impressive result from their work - their model would have been able to predict from single treatment trials what would have happened in the combination trials

February 10, 2025 at 10:48 PM
An impressive result from their work - their model would have been able to predict from single treatment trials what would have happened in the combination trials